

Burden of paediatric respiratory syncytial virus disease and potential effect of different immunisation strategies: a modelling and cost-effectiveness analysis for England
- PMID: 28804787
- PMCID: PMC5541134
- DOI: 10.1016/S2468-2667(17)30103-2
Burden of paediatric respiratory syncytial virus disease and potential effect of different immunisation strategies: a modelling and cost-effectiveness analysis for England
Abstract
Background: Vaccines and prophylactic antibodies against respiratory syncytial virus (RSV) are in development and likely to be available in the next 5-10 years. The most efficient way to use these products when they become available is an important consideration for public health decision makers.
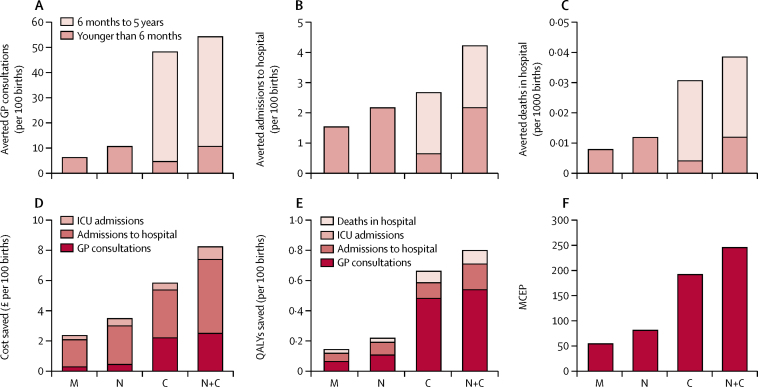
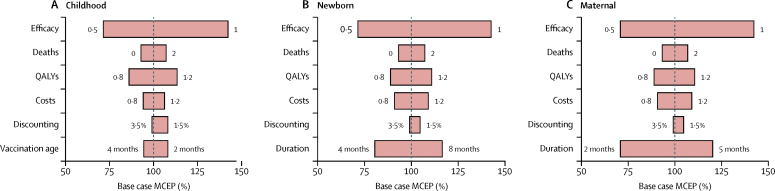
Methods: We performed a multivariate regression analysis to estimate the burden of RSV in children younger than 5 years in England (UK), a representative high-income temperate country, and used these results to assess the potential effect of different RSV immunisation strategies (targeting vaccination for infants, or pregnant women, or prophylactic antibodies for neonates). We did a cost-effectiveness analysis for these strategies, implemented either separately or concurrently, and assessed the effect of restricting vaccination to certain months of the year.
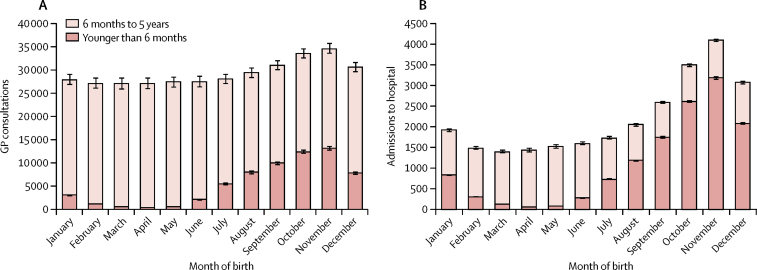
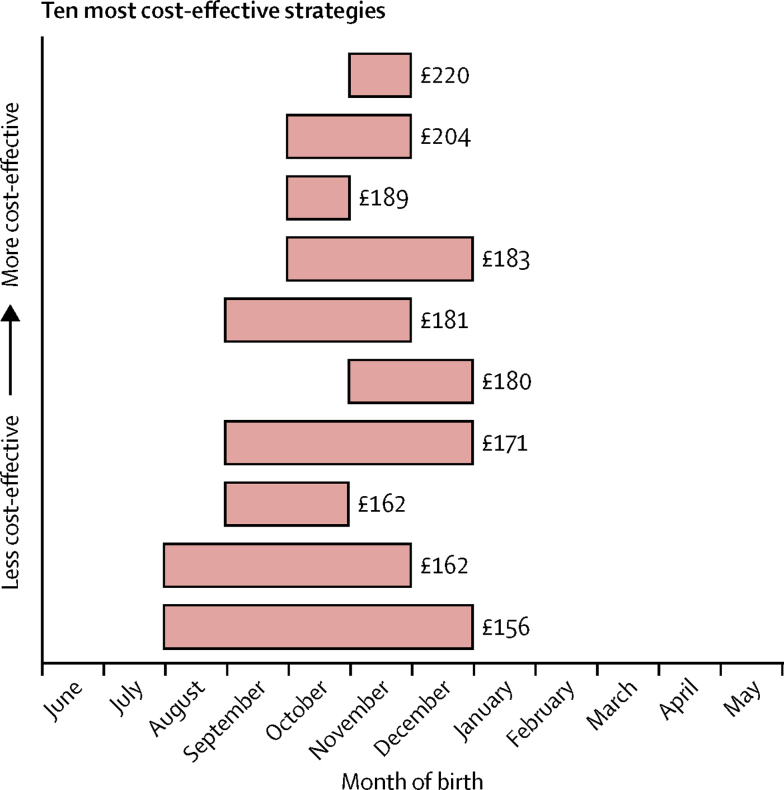
Findings: We estimated that RSV is responsible for 12 primary care consultations (95% CI 11·9-12·1) and 0·9 admissions to hospital annually per 100 children younger than 5 years (95% CI 0·89-0·90), with the major burden occurring in infants younger than 6 months. The most cost-effective strategy was to selectively immunise all children born before the start of the RSV season (maximum price of £220 [95% uncertainty interval (UI) 208-232] per vaccine, for an incremental cost-effectiveness ratio of £20 000 per quality-adjusted life-year). The maximum price per fully protected person that should be paid for the infant, newborn, and maternal strategies without seasonal restrictions was £192 (95% UI 168-219), £81 (76-86), and £54 (51-57), respectively.
Interpretation: Nearly double the number of primary care consultations, and nearly five times the number of admissions to hospital occurred with RSV compared with influenza. RSV vaccine and antibody strategies are likely to be cost-effective if they can be priced below around £200 per fully protected person. A seasonal vaccination strategy is likely to provide the most direct benefits. Herd effects might render a year-round infant vaccination strategy more appealing, although it is currently unclear whether such a programme would induce herd effects.
Funding: UK National Institute for Health Research.
Figures
Comment in
-
Seasonal immunisation against respiratory syncytial virus disease.Lancet Public Health. 2017 Aug;2(8):e344-e345. doi: 10.1016/S2468-2667(17)30122-6. Epub 2017 Jul 31. Lancet Public Health. 2017. PMID: 29253469 No abstract available.
References
-
- Teale A. Palivizumab and the importance of cost effectiveness. BMJ. 2009;338:b1935.
LinkOut - more resources
Full Text Sources
Other Literature Sources
