

A prospective study to evaluate the risk malignancy index and its diagnostic implication in patients with suspected ovarian mass
- PMID: 28806987
- PMCID: PMC5556625
- DOI: 10.1186/s13048-017-0351-2
A prospective study to evaluate the risk malignancy index and its diagnostic implication in patients with suspected ovarian mass
Abstract
Background: There is no universal screening method for discrimination between benign and malignant adnexal masses yet. Various authors have tried tumor markers, imaging studies, cytology but no one yet is a definite method for screening of cancer ovary, for which a combined diagnostic modality has come to practice in form of RMI. With this background we conducted our study "Evaluation of risk malignancy index and its diagnostic value in patients with adnexal masses".
Methods: The aim of the study was to determine the effectiveness of risk of malignancy index (RMI-3) in preoperative discrimination between benign and malignant masses and also to reveal the most suitable cut off value. We have conducted a prospective study between November 2014 to October 2016. We included the parameters like menopausal status, ultrasound features, and serum levels of tumor marker like CA-125 for calculating RMI 3. Then RMI was compared with the histopathological report which was taken as gold standard.
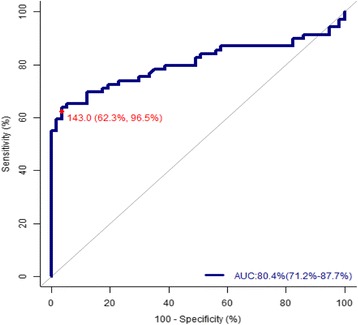
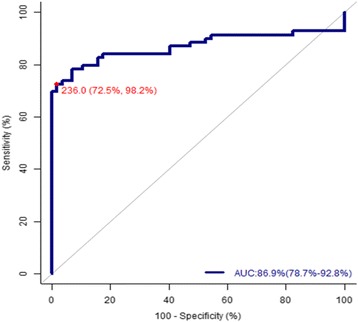
Results: In the present study malignant tumors constitute 54.76% (69/126) & benign tumors 45.24% (57/126). Bilaterality in adnexal masses and multilocularity is higher in malignant tumors than benign tumor, but a P -value >0.005 failed to be proved significant in our study. Solid area is seen in 24.69% (20/81) of benign and 75.30% (61/81) of malignant tumor. Similarly ascites was found in 38.09% (48/126) of cases. Out of which 18.75% (9/48) cases were found to be benign and malignancy was confirmed in 81.25% (39/48) patients. There is statistically significant number of malignant ovarian cancer patients where ascites and solid area is seen in USG findings (p = 0.000). Risk of Malignancy Index compared with individual parameters of Ultrasound score, CA-125 or menopausal score and a cut-off point of 236 shows a very high sensitivity (72.5%), specificity (98.2%), positive predictive value (98.1%), negative predictive value (74.7%) and diagnostic accuracy (84.13%) for discriminating malignant and benign pelvic masses.
Conclusion: Simplicity and applicability of the method in the primary evaluation of patients with pelvic masses makes it a good option in daily clinical practice in non-specialized gynecologic departments and also in developing countries where access to a gynaecologist oncologist is limited.
Keywords: Adnexal mass; Ca-125; Ovarian cancer; Risk malignancy index.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethical committee of the hospital. The aim of the study was explained appropriately and informed written consent was obtained from all the patients
Consent for publication
Permission obtained from the ethical committee and also from paticipants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Consolidated Report of Population Based Cancer Registries 2001-2004; National Cancer Registry Program. Indian Council of Medical Research Bangalore, 2006.
-
- Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG. A risk of malignancy index incorporating CA125,ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol. 1990;97(10):922–929. doi: 10.1111/j.1471-0528.1990.tb02448.x. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
