

Comparison of an alternative schedule of extended care contacts to a self-directed control: a randomized trial of weight loss maintenance
- PMID: 28806992
- PMCID: PMC5557426
- DOI: 10.1186/s12966-017-0564-1
Comparison of an alternative schedule of extended care contacts to a self-directed control: a randomized trial of weight loss maintenance
Abstract
Background: Behavioral interventions for obesity produce clinically meaningful weight loss, but weight regain following treatment is common. Extended care programs attenuate weight regain and improve weight loss maintenance. However, less is known about the most effective ways to deliver extended care, including contact schedules.
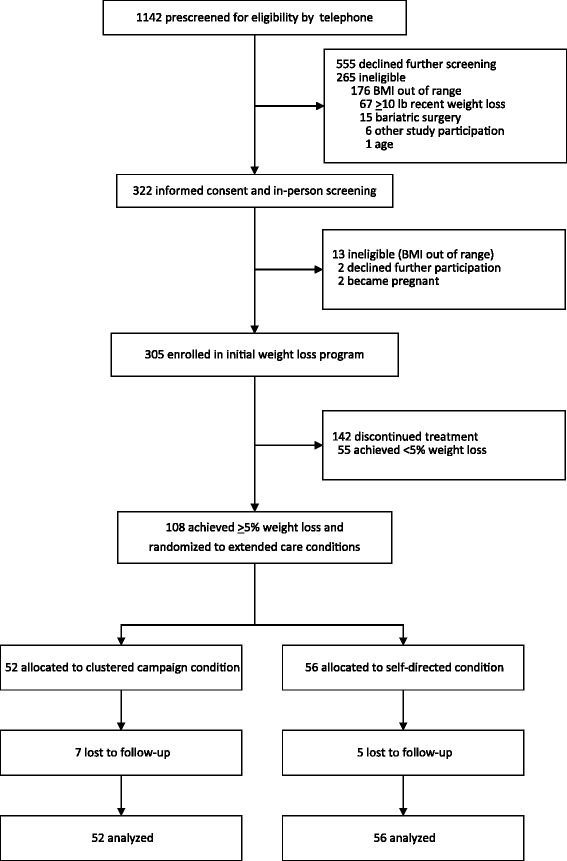
Methods: We compared the 12-month weight regain of an extended care program utilizing a non-conventional, clustered campaign treatment schedule and a self-directed program among individuals who previously achieved ≥5% weight reductions. Participants (N = 108; mean age = 51.6 years; mean weight = 92.6 kg; 52% African American; 95% female) who achieved ≥5% weight loss during an initial 16-week behavioral obesity treatment were randomized into a 2-arm, 12-month extended care trial. A clustered campaign condition included 12 group-based visits delivered in three, 4-week clusters. A self-directed condition included provision of the same printed intervention materials but no additional treatment visits. The study was conducted in a U.S. academic medical center from 2011 to 2015.
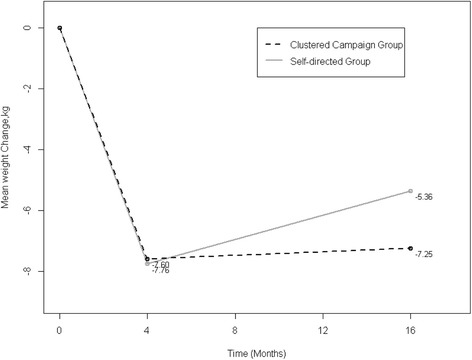
Results: Prior to randomization, participants lost an average of -7.55 ± 3.04 kg. Participants randomized to the 12-month clustered campaign program regained significantly less weight (0.35 ± 4.62 kg) than self-directed participants (2.40 ± 3.99 kg), which represented a significant between-group difference of 2.28 kg (p = 0.0154) after covariate adjustments. This corresponded to maintaining 87% and 64% of lost weight in the clustered campaign and self-directed conditions, respectively, which was a significant between-group difference of 29% maintenance of lost weight after covariate adjustments, p = 0.0396.
Conclusions: In this initial test of a clustered campaign treatment schedule, this novel approach effectively promoted 12-month maintenance of lost weight. Future trials should directly compare the clustered campaigns with conventional (e.g., monthly) extended care schedules.
Trial registration: Clinicaltrials.gov NCT02487121 . Registered 06/26/2015 (retrospectively registered).
Keywords: Adults; Behavioral treatment; Extended care; Obesity; Weight loss maintenance; Weight regain.
Conflict of interest statement
Ethics approval and consent to participate
Approval for this study was obtained from the Institutional Review Board of the participating academic health center (protocol X111215003). Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This trial is registered with
Consent for publication
Informed consent was obtained from all participants for publication of data included in this manuscript. Individual participant data, images, or video are not included in this manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, Hu FB, Hubbard VS, Jakicic JM, Kushner RF, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Obesity Society. J Am Coll Cardiol. 2014;63(25 Pt B):2985–3023. doi: 10.1016/j.jacc.2013.11.004. - DOI - PubMed
-
- Institute of Medicine (IOM) Weighing the options: Criteria for evaluating weight management programs. Washington, DC: National Academy Press; 1995. - PubMed
-
- Perri MG, Corsica JA. Improving the maintenance of weight lost in behavioral treatment of obesity. In: Wadden TA, Stunkard AJ, editors. Handbook of Obesity Treatment. New York: Guilford; 2002. pp. 357–379.
-
- Dutton GR, Perri MG. Delivery, Evaluation, and Future Directions for Cognitive Behavioral Treatments of Obesity. In: Wadden TA, Stunkard AJ, editors. The Oxford Handbook of Cognitive and Behavioral Therapies. New York: Oxford University Press; 2015. pp. 419–437.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
