

Outcomes of HIV-positive patients with cryptococcal meningitis in the Americas
- PMID: 28807740
- PMCID: PMC5649441
- DOI: 10.1016/j.ijid.2017.08.004
Outcomes of HIV-positive patients with cryptococcal meningitis in the Americas
Abstract
Background: Cryptococcal meningitis (CM) is associated with substantial mortality in HIV-infected patients. Optimal timing of antiretroviral therapy (ART) in persons with CM represents a clinical challenge, and the burden of CM in Latin America has not been well described. Studies suggest that early ART initiation is associated with higher mortality, but data from the Americas are scarce.
Methods: HIV-infected adults in care between 1985-2014 at participating sites in the Latin America (the Caribbean, Central and South America network (CCASAnet)) and the Vanderbilt Comprehensive Care Clinic (VCCC) and who had CM were included. Survival probabilities were estimated. Risk of death when initiating ART within the first 2 weeks after CM diagnosis versus initiating between 2-8 weeks was assessed using dynamic marginal structural models adjusting for site, age, sex, year of CM, CD4 count, and route of HIV transmission.
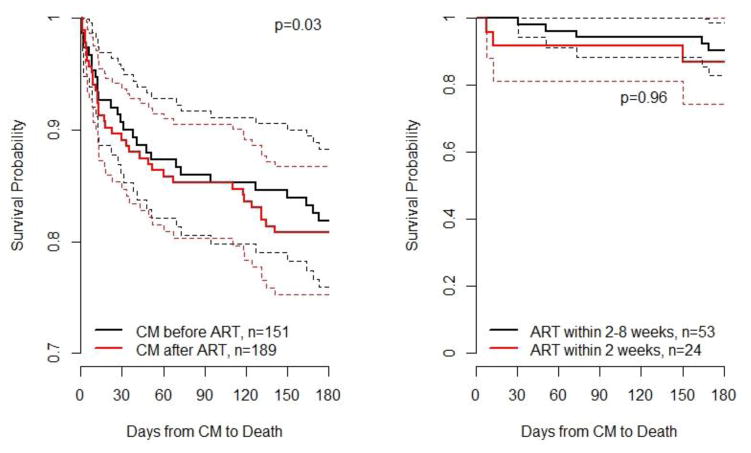
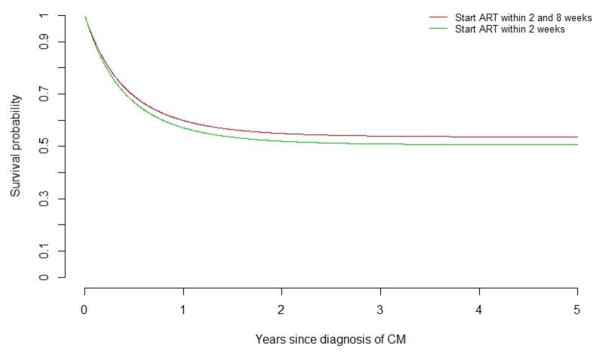
Findings: 340 patients were included (Argentina 58, Brazil 138, Chile 28, Honduras 27, Mexico 34, VCCC 55) and 142 (42%) died during the observation period. Among 151 patients with CM prior to ART 56 (37%) patients died compared to 86 (45%) of 189 with CM after ART initiation (p=0.14). Patients diagnosed with CM after ART had a higher risk of death (p=0.03, log-rank test). The probability of survival was not statistically different between patients who started ART within 2 weeks of CM (7/24, 29%) vs. those initiating between 2-8 weeks (14/53, 26%) (p=0.96), potentially due to lack of power.
Interpretation: In this large Latin-American cohort, patients with CM had very high mortality rates, especially those diagnosed after ART initiation. This study reflects the overwhelming burden of CM in HIV-infected patients in Latin America.
Keywords: AIDS; AIDS defining events; Cryptococcal meningitis; HIV; Latin America; Opportunistic Infections in HIV.
Copyright © 2017 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
B. Crabtree Ramírez, Y. Caro Vega, B.E. Shepherd, C. Le, M. Turner, P. Cahn, B. Grinsztejn, C. Cortes, D. Padgett, T.R. Sterling, C.C. McGowan and A.K. Person have no conflicts of interest to declare.
Figures
References
-
- Jarvis JN, Harrison TS. HIV-associated cryptococcal meningitis. AIDS (London, England) 2007;21:2119–2129. Editorial Review. - PubMed
-
- Bamba S, Lortholary O, Sawadogo A, et al. Decreasing incidence of cryptococcal meningitis in West Africa in the era of highly active antiretroviral therapy. AIDS (London, England) 2012;26:1039–1041. - PubMed
-
- WHO. [accessed November, 2016];Rapid advice: Diagnosis, prevention and management of cryptococcal disease in HIV-infected adults, adolescents and children. 2011 http://www.who.int/hiv/pub/cryptococcal_disease2011/en/ - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
