

Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails To Treat a Patient with a Disseminated Resistant Acinetobacter baumannii Infection
- PMID: 28807909
- PMCID: PMC5610518
- DOI: 10.1128/AAC.00954-17
Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails To Treat a Patient with a Disseminated Resistant Acinetobacter baumannii Infection
Erratum in
-
Erratum for Schooley et al., "Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails To Treat a Patient with a Disseminated Resistant Acinetobacter baumannii Infection".Antimicrob Agents Chemother. 2018 Nov 26;62(12):e02221-18. doi: 10.1128/AAC.02221-18. Print 2018 Dec. Antimicrob Agents Chemother. 2018. PMID: 30478181 Free PMC article. No abstract available.
Abstract
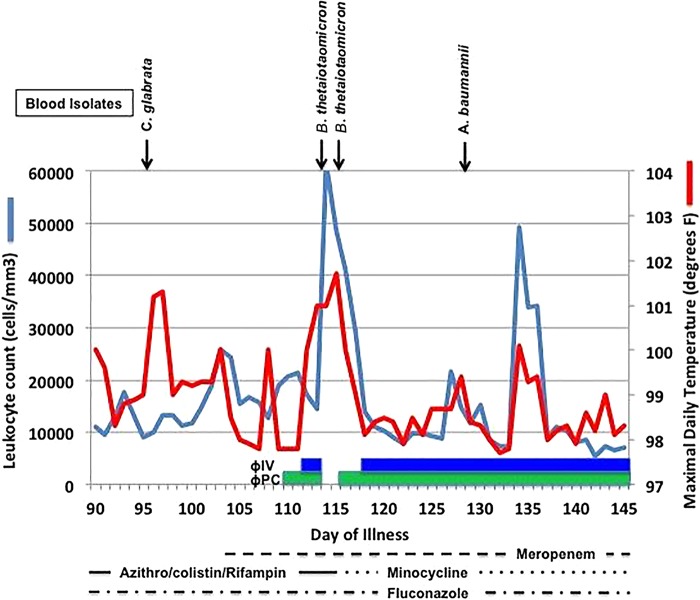
Widespread antibiotic use in clinical medicine and the livestock industry has contributed to the global spread of multidrug-resistant (MDR) bacterial pathogens, including Acinetobacter baumannii We report on a method used to produce a personalized bacteriophage-based therapeutic treatment for a 68-year-old diabetic patient with necrotizing pancreatitis complicated by an MDR A. baumannii infection. Despite multiple antibiotic courses and efforts at percutaneous drainage of a pancreatic pseudocyst, the patient deteriorated over a 4-month period. In the absence of effective antibiotics, two laboratories identified nine different bacteriophages with lytic activity for an A. baumannii isolate from the patient. Administration of these bacteriophages intravenously and percutaneously into the abscess cavities was associated with reversal of the patient's downward clinical trajectory, clearance of the A. baumannii infection, and a return to health. The outcome of this case suggests that the methods described here for the production of bacteriophage therapeutics could be applied to similar cases and that more concerted efforts to investigate the use of therapeutic bacteriophages for MDR bacterial infections are warranted.
Keywords: Acinetobacter; bacteriophage therapy; multidrug resistance.
Figures

References
-
- . 2013. Antibiotic resistance threats in the United States. Centers for Disease Control and Prevention, Atlanta, GA.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
