

Carotid Body-Mediated Chemoreflex Drive in The Setting of low and High Output Heart Failure
- PMID: 28808320
- PMCID: PMC5556057
- DOI: 10.1038/s41598-017-08142-3
Carotid Body-Mediated Chemoreflex Drive in The Setting of low and High Output Heart Failure
Abstract
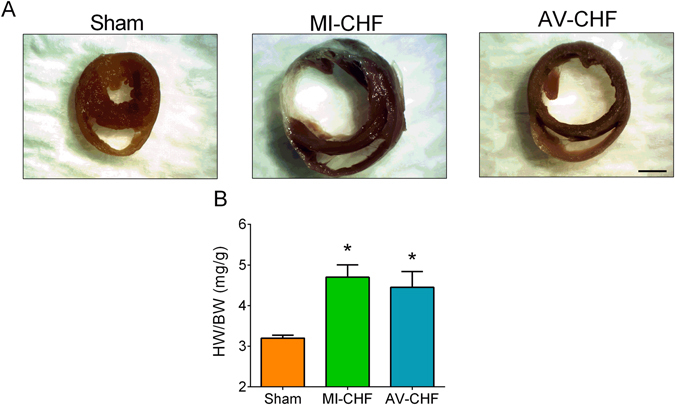
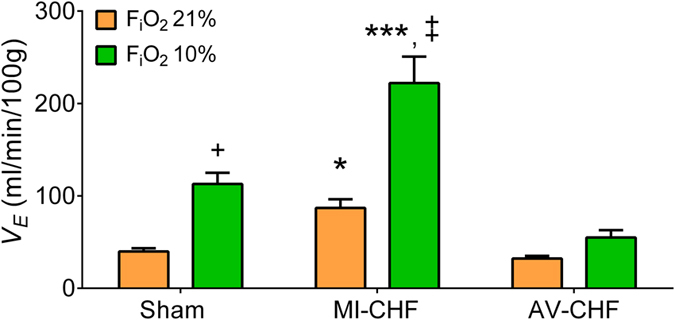
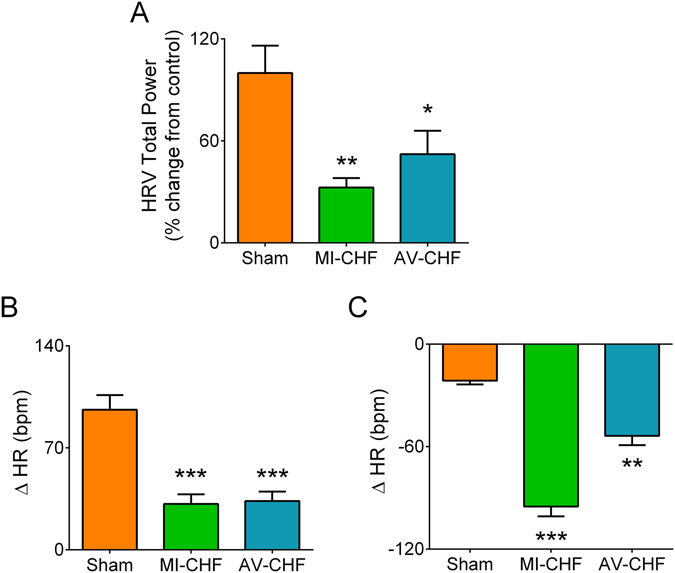
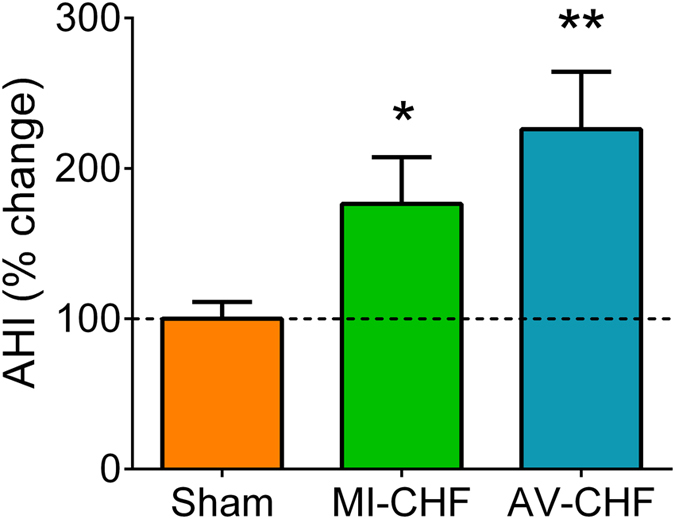
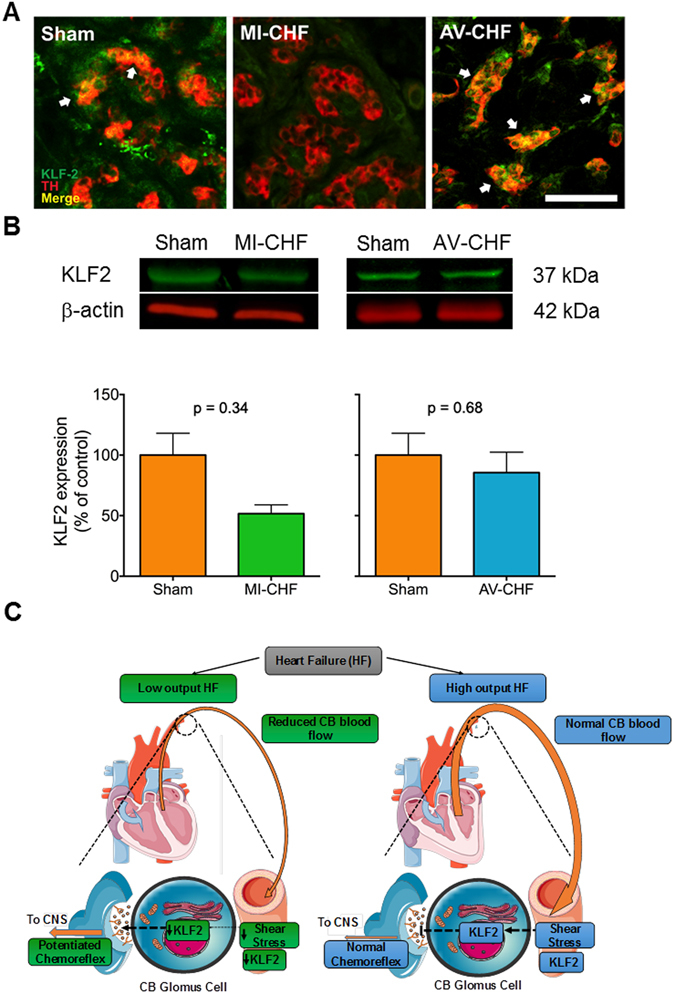
Enhanced carotid body (CB) chemoreflex function is strongly related to cardiorespiratory disorders and disease progression in heart failure (HF). The mechanisms underlying CB sensitization during HF are not fully understood, however previous work indicates blood flow per se can affect CB function. Then, we hypothesized that the CB-mediated chemoreflex drive will be enhanced only in low output HF but not in high output HF. Myocardial infarcted rats and aorto-caval fistulated rats were used as a low output HF model (MI-CHF) and as a high output HF model (AV-CHF), respectively. Blood flow supply to the CB region was decreased only in MI-CHF rats compared to Sham and AV-CHF rats. MI-CHF rats exhibited a significantly enhanced hypoxic ventilatory response compared to AV-CHF rats. However, apnea/hypopnea incidence was similarly increased in both MI-CHF and AV-CHF rats compared to control. Kruppel-like factor 2 expression, a flow sensitive transcription factor, was reduced in the CBs of MI-CHF rats but not in AV-CHF rats. Our results indicate that in the setting of HF, potentiation of the CB chemoreflex is strongly associated with a reduction in cardiac output and may not be related to other pathophysiological consequences of HF.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Swedberg K, et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115–1140. doi: 10.1093/eurheartj/ehi166. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
