

High posterior cervical fusion rates with iliac autograft and Nanoss/bone marrow aspirate
- PMID: 28808601
- PMCID: PMC5535513
- DOI: 10.4103/sni.sni_241_17
High posterior cervical fusion rates with iliac autograft and Nanoss/bone marrow aspirate
Abstract
Background: Patients with severe cervical multilevel stenosis and an adequate lordotic curvature often undergo multilevel laminectomies with posterior instrumented fusions. Although the "gold standard" for the fusion mass remains iliac crest autograft, many require additional volume provided by bone graft expanders. Here, we studied the fusion rates for 32 patients undergoing multilevel cervical laminectomy and vertex/rod/eyelet/titanium cable fusions utilizing lamina/iliac autograft and the bone graft expander Nanoss (RTI Surgical, Alachua, FL, USA) with autogenous bone marrow aspirate (BMA).
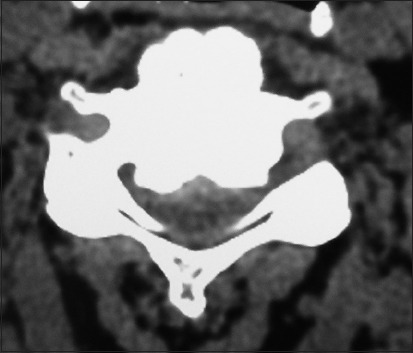
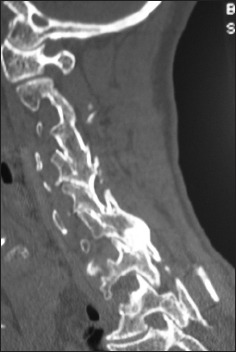
Methods: Thirty-two patients, averaging 63.0 years of age, presented with severe cervical myeloradiculopathy (average Nurick Grade 4.4). Magnetic resonance (MR) studies documented 2-3-level high intrinsic cord signals, whereas computed tomography (CT) scans confirmed marked stenosis and ossification of the posterior longitudinal ligament (OPLL)/ossification of the yellow ligament (OYL). Patients underwent multilevel lamnectomies/instrumented fusions, and were followed up for an average of 2.7 years.
Results: Multilevel laminectomies (2.8 levels) and average 7.8-level vertex/rod/eyelet/cable fusions were performed utilizing lamina/iliac crest autograft and Nanoss/BMA. Fusion was confirmed on X-ray/CT studies an average of 4.7 months postoperatively in 31 of 32 patients (97%); there was just one pseudarthrosis requiring secondary surgery. The only other complication was a delayed transient C5 palsy that fully resolved in 6 postoperative months.
Conclusions: Thirty-two severely myelopathic underwent 2.8-level cervical laminectomies/7.8 level fusions utilizing lamina/iliac autograft and Nanoss/BMA. Fusion was documented on both dynamic X-ray and CT studies in 31 of 32 (97%) patients an average of 4.7 months postoperatively. Nanoss/BMA appears to be a safe and effective bone graft expander that can be utilized for posterior cervical fusions.
Keywords: Bone graft expander; Nanoss; bone marrow aspirate (BMA); high fusion rates; posterior cervical fusions.
Conflict of interest statement
There are no conflicts of interest.
Figures






Similar articles
-
High lumbar noninstrumented fusion rates using lamina autograft and Nanoss/bone marrow aspirate.Surg Neurol Int. 2017 Jul 20;8:153. doi: 10.4103/sni.sni_248_17. eCollection 2017. Surg Neurol Int. 2017. PMID: 28808602 Free PMC article.
-
Preliminary documentation of the comparable efficacy of vitoss versus NanOss bioactive as bone graft expanders for posterior cervical fusion.Surg Neurol Int. 2015 May 7;6(Suppl 4):S164-71. doi: 10.4103/2152-7806.156559. eCollection 2015. Surg Neurol Int. 2015. PMID: 26005578 Free PMC article.
-
Preliminary study showing safety/efficacy of nanoss bioactive versus vitoss as bone graft expanders for lumbar noninstrumented fusions.Surg Neurol Int. 2015 Jun 25;6(Suppl 10):S318-22. doi: 10.4103/2152-7806.159380. eCollection 2015. Surg Neurol Int. 2015. PMID: 26167369 Free PMC article.
-
Anterior approaches to cervical spondylosis and ossification of the posterior longitudinal ligament: review of operative technique and assessment of 65 multilevel circumferential procedures.Surg Neurol. 2001 Jun;55(6):313-24. doi: 10.1016/s0090-3019(01)00464-5. Surg Neurol. 2001. PMID: 11483184 Review.
-
[Diagnosis and management of ossification of the posterior longitudinal ligament of the cervical spine].Brain Nerve. 2009 Nov;61(11):1343-50. Brain Nerve. 2009. PMID: 19938692 Review. Japanese.
Cited by
-
Nursing review of cervical laminectomy and fusion.Surg Neurol Int. 2017 Dec 11;8:300. doi: 10.4103/sni.sni_243_17. eCollection 2017. Surg Neurol Int. 2017. PMID: 29296286 Free PMC article.
-
Evaluation of Vertebral Function and Long-Term Quality of Life after Percutaneous Minimally Invasive Surgery in Patients with Thoracolumbar Spine Fractures.Comput Math Methods Med. 2022 Feb 23;2022:2723542. doi: 10.1155/2022/2723542. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Sep 27;2023:9859432. doi: 10.1155/2023/9859432. PMID: 35251297 Free PMC article. Retracted. Clinical Trial.
-
Clinical and radiological outcomes of a cervical cage with integrated fixation.Medicine (Baltimore). 2019 Jan;98(3):e14097. doi: 10.1097/MD.0000000000014097. Medicine (Baltimore). 2019. PMID: 30653129 Free PMC article.
-
A feasibility study of modified self-efficacy for the improvement of adverse emotions and quality of life in traumatic fracture patients.Am J Transl Res. 2021 Jun 15;13(6):6507-6515. eCollection 2021. Am J Transl Res. 2021. PMID: 34306391 Free PMC article.
-
Autologous Stem Cells in Cervical Spine Fusion.Global Spine J. 2021 Jul;11(6):950-965. doi: 10.1177/2192568220948479. Epub 2020 Sep 23. Global Spine J. 2021. PMID: 32964752 Free PMC article.
References
-
- Baumann F, Krutsch W, Pfeifer C, Neumann C, Nerlich M, Loibl M. Posterolateral fusion in acute traumatic thoracolumbar fractures: A comparison of demineralized bone matrix and autologous bone graft. Acta Chir Orthop Traumatol Cech. 2015;82:119–25. - PubMed
-
- Epstein NE. A preliminary study of the efficacy of Beta Tricalcium Phosphate as a bone expander for instrumented posterolateral lumbar fusions. J Spinal Disord Tech. 2006;19:424–9. - PubMed
-
- Epstein NE. Efficacy of different bone volume expanders for augmenting lumbar fusions. Surg Neurol. 2008;69:16–9. discussion 19. - PubMed
-
- Epstein NE. An argument for traditional posterior cervical fusion techniques: Evidence from 35 cases. Surg Neurol. 2008;70:45–51. discussion 51-2. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous