

Utilization and predictors of expectant management among elderly men with low-and intermediate-risk localized prostate cancer in U.S. urological practice
- PMID: 28808670
- PMCID: PMC5553913
- DOI: 10.1016/j.urpr.2016.05.005
Utilization and predictors of expectant management among elderly men with low-and intermediate-risk localized prostate cancer in U.S. urological practice
Abstract
Introduction: Expectant management (EM) reduces overtreatment in low-risk but not intermediate-risk localized prostate cancer (PCa). We assessed the use and predictors of EM to understand its uptake in U.S. practice.
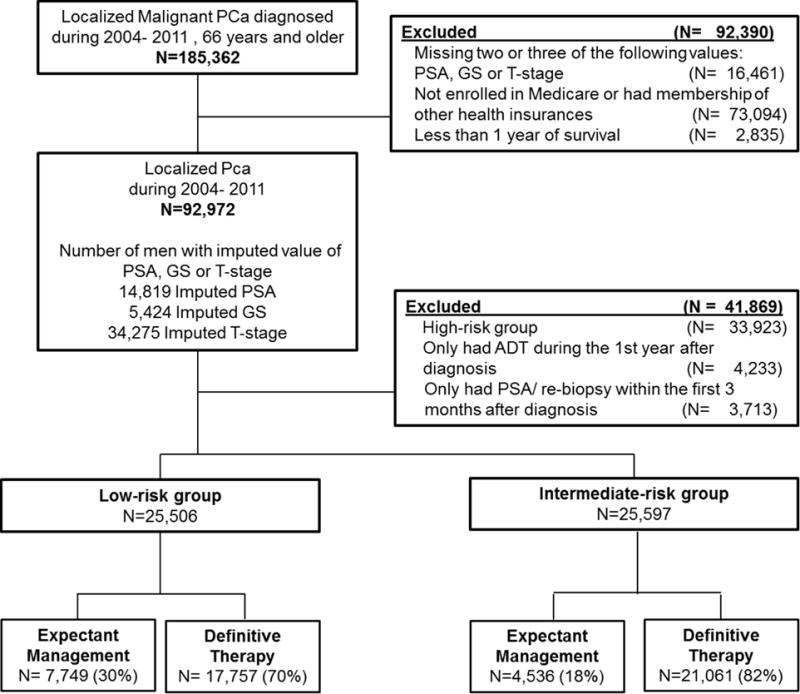
Methods: Using the U.S. SEER-Medicare database, we conducted a retrospective cohort study of men 66 years and older diagnosed with low-risk (N=25,506) or intermediate-risk (N=25,597) localized PCa between 2004 - 2011 and followed through December 31, 2012. We defined EM as no definitive therapy (DT) and at least one prostate-specific antigen (PSA) test or re-biopsy 4 - 12 months post diagnosis; or receiving DT after PSA testing or re-biopsy 7 - 12 months after diagnosis. We performed separate analyses for low-risk and intermediate-risk groups using multiple logistic regressions.
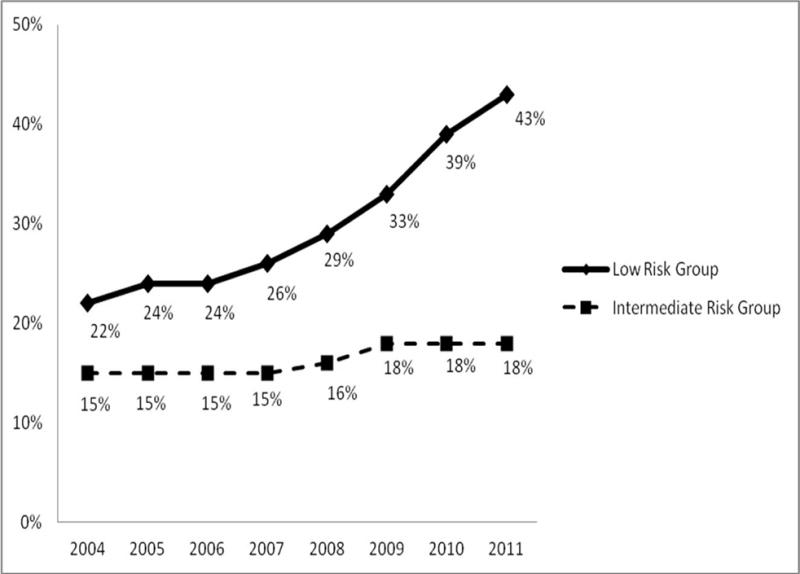
Results: For men diagnosed with PCa in 2004-2011, EM increased from 22% to 43% in the low-risk group and from 15% to 18% in the intermediate-risk group. In the low-risk group, EM increased with patients' age (adjusted odds ratio [aOR] = 1.26 for 71-75 years; 2.21 for 76-80 years; 6.33 for older then 80, p<0.0001, compared to 66-70 years). EM uptake was higher among men with comorbidities (aOR=1.29), and residing in the Pacific region (aOR=0.56, compared to the East Coast).
Conclusions: In U.S. practice, the utilization of EM steadily increased in low-risk PCa and remained low in the intermediate-risk group over time. While patients with advanced age or comorbidities were more likely to receive EM, its use varied substantially by geographic region. Our findings bring attention to the presence of multiple barriers for EM implementation.
Keywords: prostatic neoplasms; utilization.
Conflict of interest statement
Conflict of interest: none.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2016. Updated 2016. Accessed 2016 Feb 18. http://www.cancer.org/acs/groups/content/@research/documents/document/ac....
-
- National Cancer Institute. SEER Cancer Statistics Review, 1975–2006. Updated 2009. Accessed 2013 Dec 5. http://seer.cancer.gov/csr/1975_2006.
-
- Popiolek M, Rider JR, Andren O, et al. Natural history of early, localized prostate cancer: a final report from three decades of follow-up. Eur Urol. 2013 Mar;63(3):428–35. - PubMed
-
- Punnen S, Cowan JE, Chan JM, et al. Long-term Health-related Quality of Life After Primary Treatment for Localized Prostate Cancer: Results from the CaPSURE Registry. Eur Urol. 2015 Oct;68(4):600–8. - PubMed
-
- Jarosek SL, Virnig BA, Chu H, et al. Propensity-weighted long-term risk of urinary adverse events after prostate cancer surgery, radiation, or both. Eur Urol. 2015 Feb;67(2):273–80. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
