

Lymphopaenia in cardiac arrest patients
- PMID: 28808927
- PMCID: PMC5555958
- DOI: 10.1186/s13613-017-0308-z
Lymphopaenia in cardiac arrest patients
Abstract
Background: A decrease in circulating lymphocytes has been described as a marker of poor prognosis after septic shock; however, scarce data are available after cardiac arrest (CA). The aim of this study was to evaluate the impact of lymphopaenia after successful cardiopulmonary resuscitation.
Methods: This is a retrospective analysis of an institutional database including all adult CA patients admitted to the intensive care unit (ICU) between January 2007 and December 2014 who survived for at least 24 h. Demographic, CA-related data and ICU mortality were recorded as was lymphocyte count on admission and for the first 48 h. A cerebral performance category score of 3-5 at 3 months was considered as an unfavourable neurological outcome.
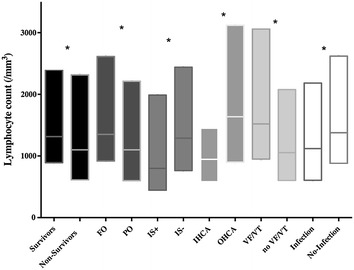
Results: Data from 377 patients were analysed (median age: 62 [IQRs: 52-75] years). Median time to return of spontaneous circulation (ROSC) was 15 [8-25] min and 232 (62%) had a non-shockable initial rhythm. ICU mortality was 58% (n = 217) and 246 (65%) patients had an unfavourable outcome at 3 months. The median lymphocyte count on admission was 1208 [700-2350]/mm3 and 151 (40%) patients had lymphopaenia (lymphocyte count <1000/mm3). Predictors of lymphopaenia on admission were older age, a shorter time to ROSC, prior use of corticosteroid therapy and high C-reactive protein levels on admission. ICU non-survivors had lower lymphocyte counts on admission than survivors (1100 [613-2317] vs. 1316 [891-2395]/mm3; p = 0.05) as did patients with unfavourable compared to those with favourable neurological outcomes (1100 [600-2013] vs. 1350 [919-2614]/mm3; p = 0.003). However, lymphopaenia on admission was not an independent predictor of poor outcomes in the entire population, but only among OHCA patients.
Conclusions: A low lymphocyte count is common in CA survivors and is associated with poor outcome after OHCA.
Keywords: Cardiac arrest; Lymphopaenia; Outcome; Prognosis.
Figures

References
-
- Neumar RW, Nolan JP, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication: a consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, Inter American Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–2483. doi: 10.1161/CIRCULATIONAHA.108.190652. - DOI - PubMed
-
- Adrie C, Adib-Conquy M, Laurent I, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106(5):562–568. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
