

Treatment of Patients With Metastatic Cancer Using a Major Histocompatibility Complex Class II-Restricted T-Cell Receptor Targeting the Cancer Germline Antigen MAGE-A3
- PMID: 28809608
- PMCID: PMC5652397
- DOI: 10.1200/JCO.2017.74.5463
Treatment of Patients With Metastatic Cancer Using a Major Histocompatibility Complex Class II-Restricted T-Cell Receptor Targeting the Cancer Germline Antigen MAGE-A3
Abstract
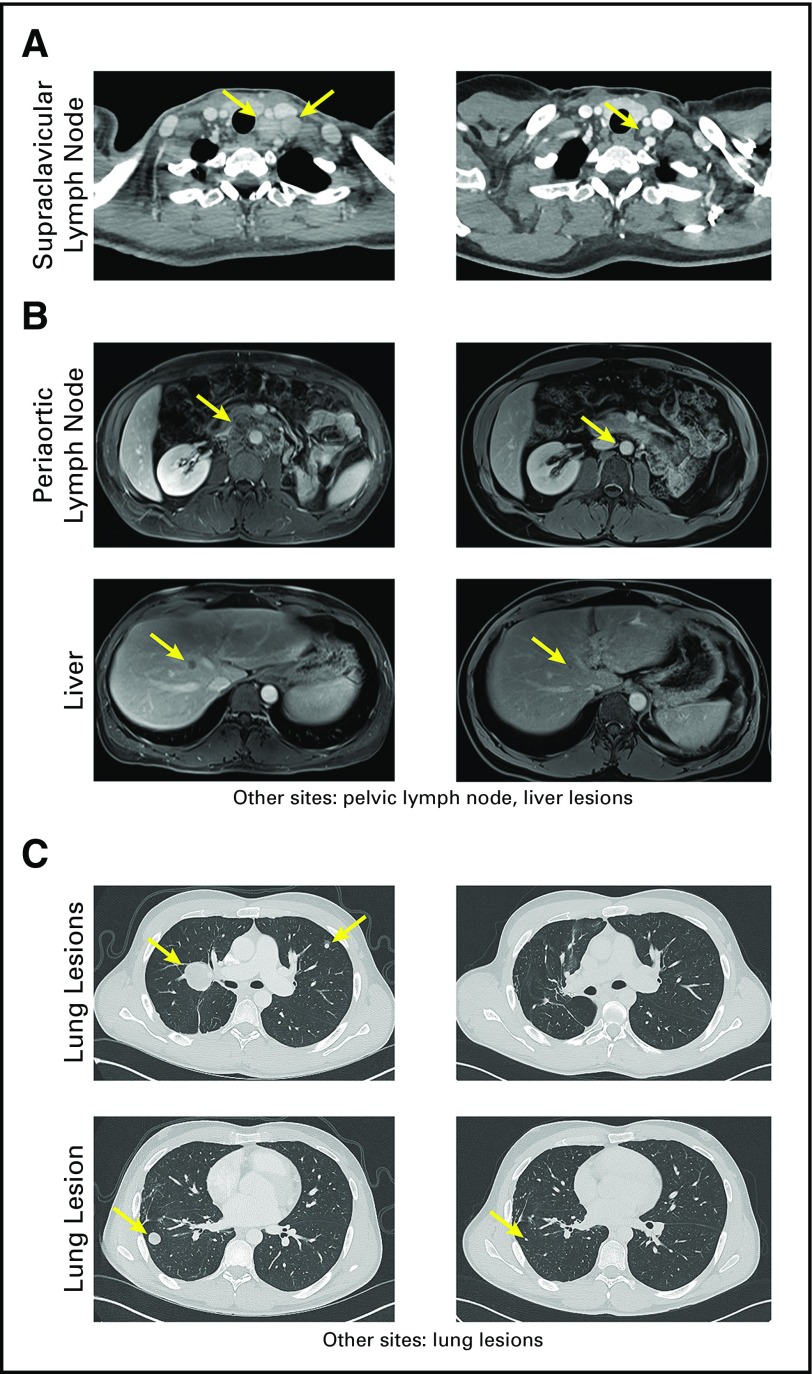
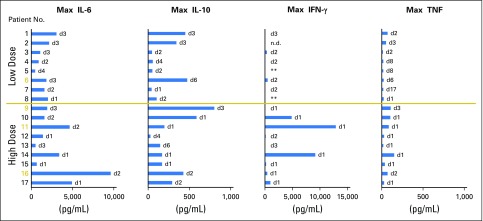
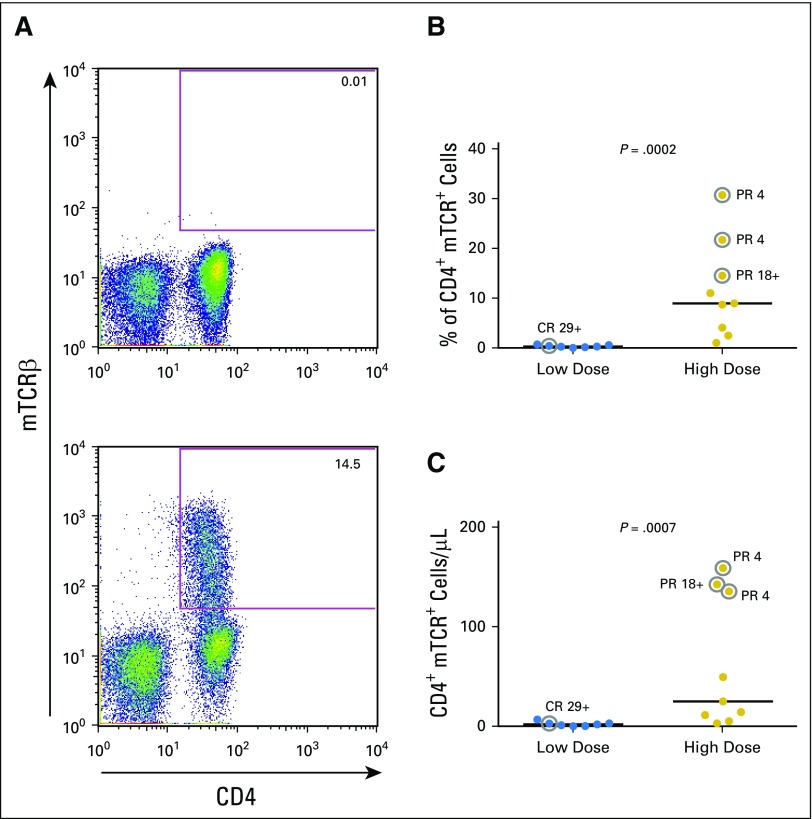
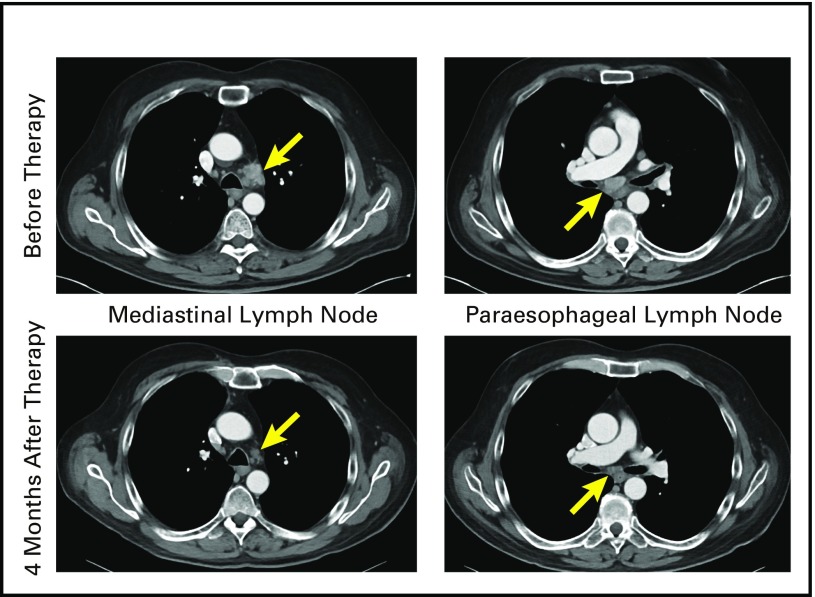
Purpose Adoptive transfer of genetically modified T cells is being explored as a treatment for patients with metastatic cancer. Most current strategies use genes that encode major histocompatibility complex (MHC) class I-restricted T-cell receptors (TCRs) or chimeric antigen receptors to genetically modify CD8+ T cells or bulk T cells for treatment. Here, we evaluated the safety and efficacy of an adoptive CD4+ T-cell therapy using an MHC class II-restricted, HLA-DPB1*0401-restricted TCR that recognized the cancer germline antigen, MAGE-A3 (melanoma-associated antigen-A3). Patients and Methods Patients received a lymphodepleting preparative regimen, followed by adoptive transfer of purified CD4+ T cells, retrovirally transduced with MAGE-A3 TCR plus systemic high-dose IL-2. A cell dose escalation was conducted, starting at 107 total cells and escalating at half-log increments to approximately 1011 cells. Nine patients were treated at the highest dose level (0.78 to 1.23 × 1011 cells). Results Seventeen patients were treated. During the cell dose-escalation phase, an objective complete response was observed in a patient with metastatic cervical cancer who received 2.7 × 109 cells (ongoing at ≥ 29 months). Among nine patients who were treated at the highest dose level, objective partial responses were observed in a patient with esophageal cancer (duration, 4 months), a patient with urothelial cancer (ongoing at ≥ 19 months), and a patient with osteosarcoma (duration, 4 months). Most patients experienced transient fevers and the expected hematologic toxicities from lymphodepletion pretreatment. Two patients experienced transient grade 3 and 4 transaminase elevations. There were no treatment-related deaths. Conclusion These results demonstrate the safety and efficacy of administering autologous CD4+ T cells that are genetically engineered to express an MHC class II-restricted antitumor TCR that targets MAGE-A3. This clinical trial extends the reach of TCR gene therapy for patients with metastatic cancer.
Figures
Similar articles
-
Isolation and Characterization of an HLA-DPB1*04: 01-restricted MAGE-A3 T-Cell Receptor for Cancer Immunotherapy.J Immunother. 2016 Jun;39(5):191-201. doi: 10.1097/CJI.0000000000000123. J Immunother. 2016. PMID: 27163739 Free PMC article.
-
Redirecting human CD4+ T lymphocytes to the MHC class I-restricted melanoma antigen MAGE-A1 by TCR alphabeta gene transfer requires CD8alpha.Gene Ther. 2005 Jan;12(2):140-6. doi: 10.1038/sj.gt.3302388. Gene Ther. 2005. PMID: 15496961
-
TCR gene transfer: MAGE-C2/HLA-A2 and MAGE-A3/HLA-DP4 epitopes as melanoma-specific immune targets.Clin Dev Immunol. 2012;2012:586314. doi: 10.1155/2012/586314. Epub 2012 Feb 12. Clin Dev Immunol. 2012. PMID: 22400038 Free PMC article.
-
Melanoma-associated antigen A4: A cancer/testis antigen as a target for adoptive T-cell receptor T-cell therapy.Cancer Treat Rev. 2025 Mar;134:102891. doi: 10.1016/j.ctrv.2025.102891. Epub 2025 Jan 26. Cancer Treat Rev. 2025. PMID: 39970827 Review.
-
MHC class II restricted neoantigen: A promising target in tumor immunotherapy.Cancer Lett. 2017 Apr 28;392:17-25. doi: 10.1016/j.canlet.2016.12.039. Epub 2017 Jan 16. Cancer Lett. 2017. PMID: 28104443 Review.
Cited by
-
Impact of Immunotherapy on CD4 T Cell Phenotypes and Function in Cancer.Vaccines (Basel). 2021 May 4;9(5):454. doi: 10.3390/vaccines9050454. Vaccines (Basel). 2021. PMID: 34064410 Free PMC article. Review.
-
Targeting the melanoma-associated antigen CSPG4 with HLA-C*07:01-restricted T-cell receptors.Front Immunol. 2023 Oct 2;14:1245559. doi: 10.3389/fimmu.2023.1245559. eCollection 2023. Front Immunol. 2023. PMID: 37849763 Free PMC article.
-
Chimeric antigen receptor-modified T cells: CD19 and the road beyond.Blood. 2018 Jun 14;131(24):2621-2629. doi: 10.1182/blood-2018-01-785840. Epub 2018 May 4. Blood. 2018. PMID: 29728402 Free PMC article. Review.
-
Identifying and Targeting Human Tumor Antigens for T Cell-Based Immunotherapy of Solid Tumors.Cancer Cell. 2020 Oct 12;38(4):454-472. doi: 10.1016/j.ccell.2020.07.013. Epub 2020 Aug 20. Cancer Cell. 2020. PMID: 32822573 Free PMC article. Review.
-
Engineered Adoptive T-Cell Therapies for Breast Cancer: Current Progress, Challenges, and Potential.Cancers (Basel). 2023 Dec 26;16(1):124. doi: 10.3390/cancers16010124. Cancers (Basel). 2023. PMID: 38201551 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
