

Effect of tolvaptan on renal handling of water and sodium, GFR and central hemodynamics in autosomal dominant polycystic kidney disease during inhibition of the nitric oxide system: a randomized, placebo-controlled, double blind, crossover study
- PMID: 28810844
- PMCID: PMC5558668
- DOI: 10.1186/s12882-017-0686-3
Effect of tolvaptan on renal handling of water and sodium, GFR and central hemodynamics in autosomal dominant polycystic kidney disease during inhibition of the nitric oxide system: a randomized, placebo-controlled, double blind, crossover study
Abstract
Background: Tolvaptan slows progression of autosomal dominant polycystic kidney disease (ADPKD) by antagonizing the vasopressin-cAMP axis. Nitric oxide (NO) stimulates natriuresis and diuresis, but its role is unknown during tolvaptan treatment in ADPKD.
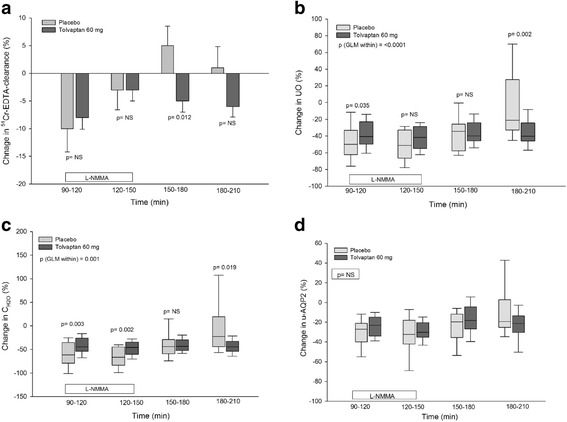
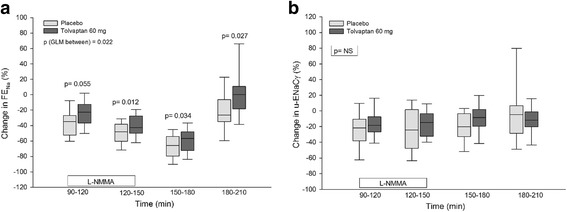
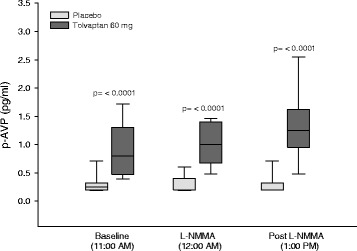
Methods: Eighteen patients with ADPKD received tolvaptan 60 mg or placebo in a randomized, placebo-controlled, double blind, crossover study. L-NMMA (L-NG-monomethyl-arginine) was given as a bolus followed by continuous infusion during 60 min. We measured: GFR, urine output (UO), free water clearance (CH2O), fractional excretion of sodium (FENa), urinary excretion of aquaporin-2 channels (u-AQP2) and epithelial sodium channels (u-ENaCγ), plasma concentrations of vasopressin (p-AVP), renin (PRC), angiotensinII (p-AngII), aldosterone (p-Aldo), and central blood pressure (cBP).
Results: During tolvaptan with NO-inhibition, a more pronounced decrease was measured in UO, CH2O (61% vs 43%) and FENa (46% vs 41%) after placebo than after tolvaptan; GFR and u-AQP2 decreased to the same extent; p-AVP increased three fold, whereas u-ENaCγ, PRC, p-AngII, and p-Aldo remained unchanged. After NO-inhibition, GFR increased after placebo and remained unchanged after tolvaptan (5% vs -6%). Central diastolic BP (CDBP) increased to a higher level after placebo than tolvaptan. Body weight fell during tolvaptan treatment.
Conclusions: During NO inhibition, tolvaptan antagonized both the antidiuretic and the antinatriuretic effect of L-NMMA, partly via an AVP-dependent mechanism. U-AQP2 was not changed by tolvaptan, presumeably due to a counteracting effect of elevated p-AVP. The reduced GFR during tolvaptan most likely is caused by the reduction in extracellular fluid volume and blood pressure.
Trial registration: Clinical Trial no: NCT02527863 . Registered 18 February 2015.
Keywords: ADPKD; AQP2; Blood pressure; ENaC; Nitric oxide; Tolvaptan; Vasoactive hormones.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by The Central Denmark Region Committees on Health Research Ethics (Clinical Trial no: NCT02527863). The study was conducted in conformity with the principles of the declaration of Helsinki. Written informed consent was obtained from all subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Devuyst O, Knoers NV, Remuzzi G, Schaefer F. Board of the Working Group for inherited kidney diseases of the European Renal Association and European dialysis and transplant association. Rare inherited kidney diseases: challenges, opportunities, and perspectives. Lancet. 2014;383(9931):1844–1859. doi: 10.1016/S0140-6736(14)60659-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
