

Epidemiology of Clostridium difficile in infants in Oxfordshire, UK: Risk factors for colonization and carriage, and genetic overlap with regional C. difficile infection strains
- PMID: 28813461
- PMCID: PMC5559064
- DOI: 10.1371/journal.pone.0182307
Epidemiology of Clostridium difficile in infants in Oxfordshire, UK: Risk factors for colonization and carriage, and genetic overlap with regional C. difficile infection strains
Abstract
Background: Approximately 30-40% of children <1 year of age are Clostridium difficile colonized, and may represent a reservoir for adult C. difficile infections (CDI). Risk factors for colonization with toxigenic versus non-toxigenic C. difficile strains and longitudinal acquisition dynamics in infants remain incompletely characterized.
Methods: Predominantly healthy infants (≤2 years) were recruited in Oxfordshire, UK, and provided ≥1 fecal samples. Independent risk factors for toxigenic/non-toxigenic C. difficile colonization and acquisition were identified using multivariable regression. Infant C. difficile isolates were whole-genome sequenced to assay genetic diversity and prevalence of toxin-associated genes, and compared with sequenced strains from Oxfordshire CDI cases.
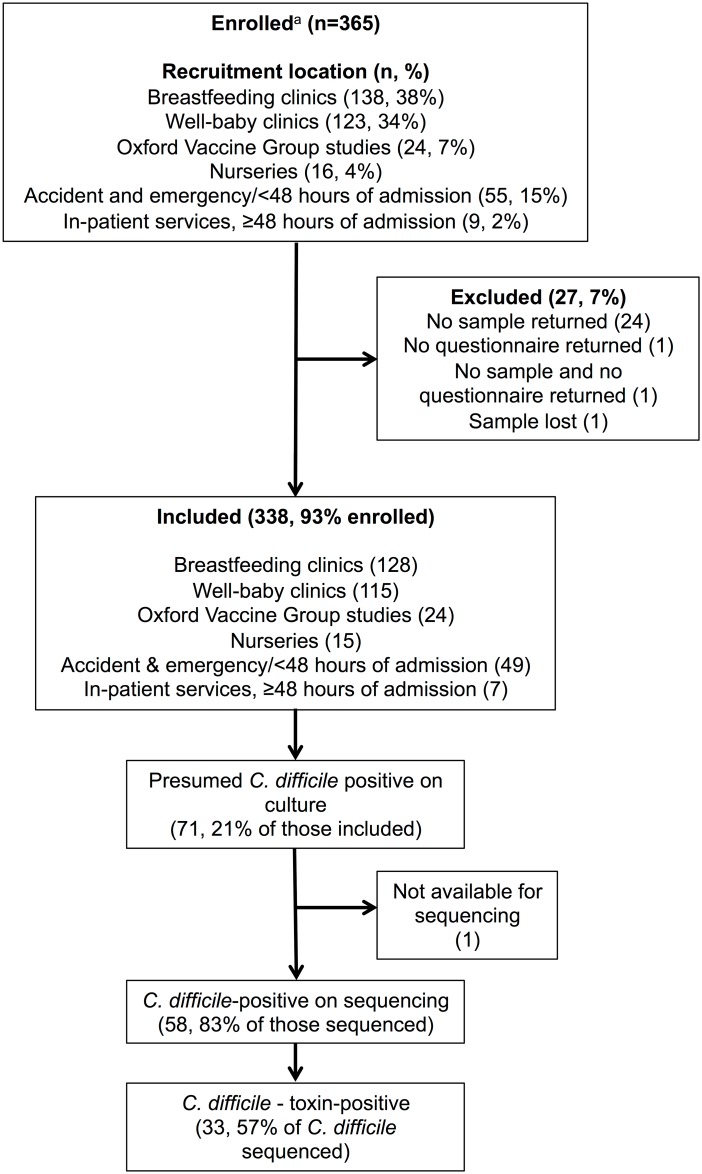
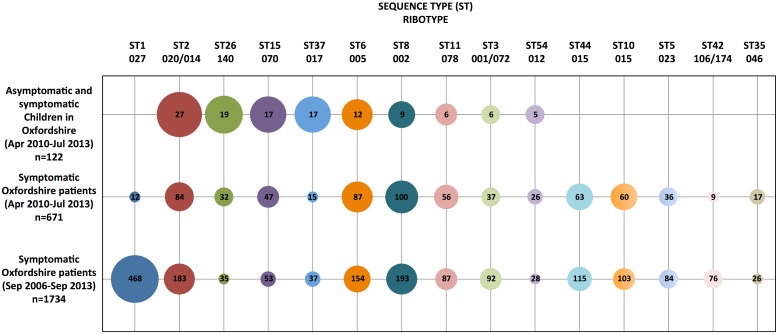
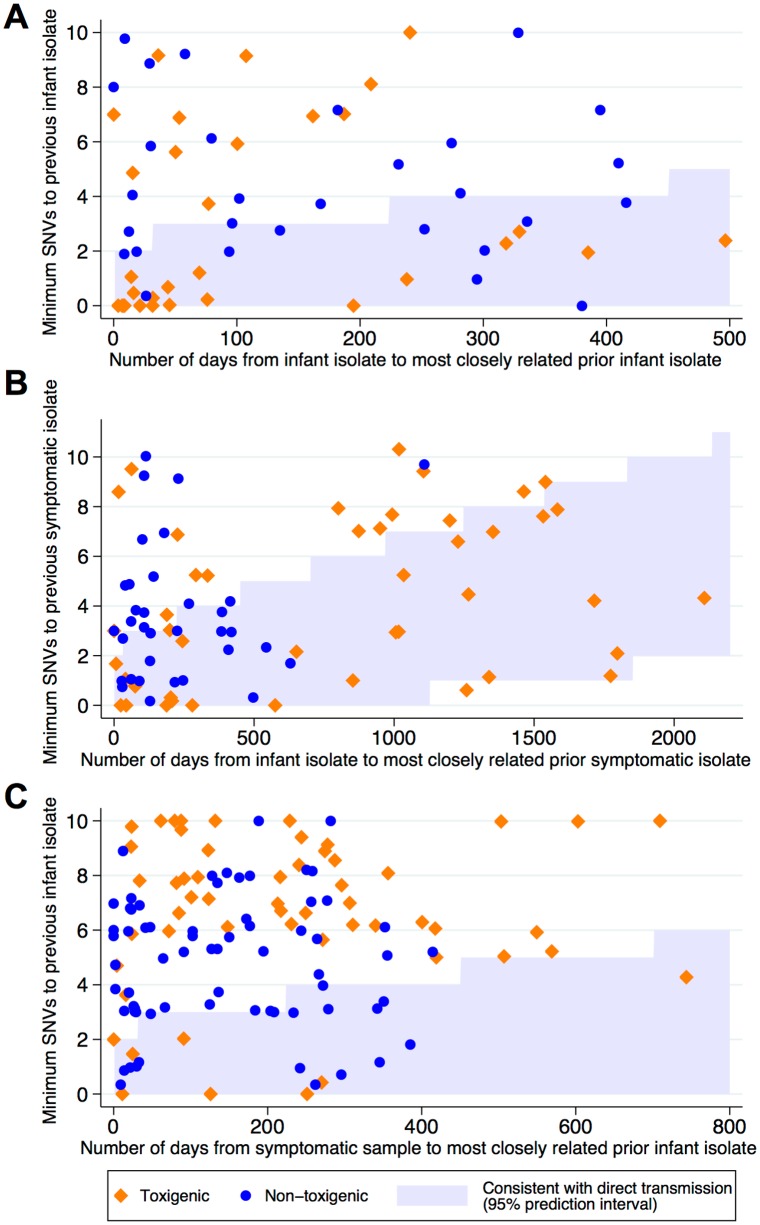
Results: 338/365 enrolled infants provided 1332 fecal samples, representing 158 C. difficile colonization or carriage episodes (107[68%] toxigenic). Initial colonization was associated with age, and reduced with breastfeeding but increased with pet dogs. Acquisition was associated with older age, Caesarean delivery, and diarrhea. Breastfeeding and pre-existing C. difficile colonization reduced acquisition risk. Overall 13% of CDI C. difficile strains were genetically related to infant strains. 29(18%) infant C. difficile sequences were consistent with recent direct/indirect transmission to/from Oxfordshire CDI cases (≤2 single nucleotide variants [SNVs]); 79(50%) shared a common origin with an Oxfordshire CDI case within the last ~5 years (0-10 SNVs). The hypervirulent, epidemic ST1/ribotype 027 remained notably absent in infants in this large study, as did other lineages such as STs 10/44 (ribotype 015); the most common strain in infants was ST2 (ribotype 020/014)(22%).
Conclusions: In predominantly healthy infants without significant healthcare exposure C. difficile colonization and acquisition reflect environmental exposures, with pet dogs identified as a novel risk factor. Genetic overlap between some infant strains and those isolated from CDI cases suggest common community reservoirs of these C. difficile lineages, contrasting with those lineages found only in CDI cases, and therefore more consistent with healthcare-associated spread.
Conflict of interest statement
Figures
References
-
- Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372(16):1539–48. doi: 10.1056/NEJMra1403772 . - DOI - PubMed
-
- Evans CT, Safdar N. Current Trends in the Epidemiology and Outcomes of Clostridium difficile Infection. Clin Infect Dis. 2015;60 Suppl 2:S66–71. doi: 10.1093/cid/civ140 . - DOI - PubMed
-
- Gupta A, Khanna S. Community-acquired Clostridium difficile infection: an increasing public health threat. Infect Drug Resist. 2014;7:63–72. doi: 10.2147/IDR.S46780 . - DOI - PMC - PubMed
-
- Enoch DA, Butler MJ, Pai S, Aliyu SH, Karas JA. Clostridium difficile in children: colonisation and disease. J Infect. 2011;63(2):105–13. doi: 10.1016/j.jinf.2011.05.016 . - DOI - PubMed
-
- Stoesser N, Crook DW, Fung R, Griffiths D, Harding RM, Kachrimanidou M, et al. Molecular epidemiology of Clostridium difficile strains in children compared with that of strains circulating in adults with Clostridium difficile-associated infection. J Clin Microbiol. 2011;49(11):3994–6. doi: 10.1128/JCM.05349-11 . - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
