

Implementation of a comprehensive intervention for patients at high risk of cardiovascular disease in rural China: A pragmatic cluster randomized controlled trial
- PMID: 28813512
- PMCID: PMC5559073
- DOI: 10.1371/journal.pone.0183169
Implementation of a comprehensive intervention for patients at high risk of cardiovascular disease in rural China: A pragmatic cluster randomized controlled trial
Abstract
Objective: This study aims to assess whether a standard intervention package of cardiovascular disease (CVD) care was being delivered effectively, and if it was associated with improved lifestyle and biomedical indicators.
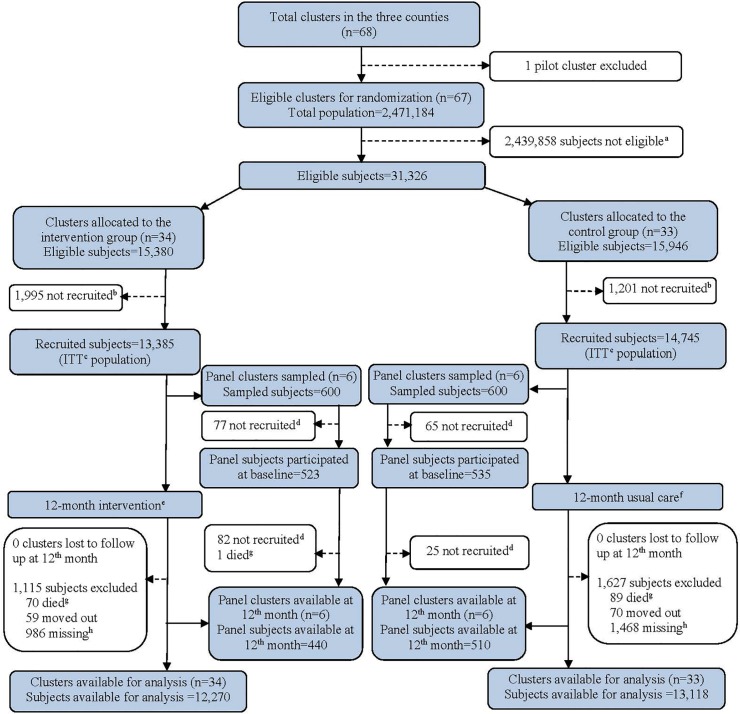
Methods: In rural China, we implemented a pragmatic cluster randomized controlled trial for 12 months, randomized at the township hospital level, and compared with usual care. Intervention case management guideline, training and performance monitoring meeting and patient support activities were designed to fit within the job description of family doctors in the township hospitals and comprised: 1) prescription of a standardised package of medicines targeted at those with hypertension or diabetes; 2) advice about specific lifestyle interventions; and 3) advice about medication adherence. Participants were 50-74 years old, had hypertension and CVD risk scores >20% or diabetes, but were excluded if a history of severe CVD events. We also randomly selected 100 participants from six selected clusters per arm as a panel to collect intermediate biomedical indicators over time.
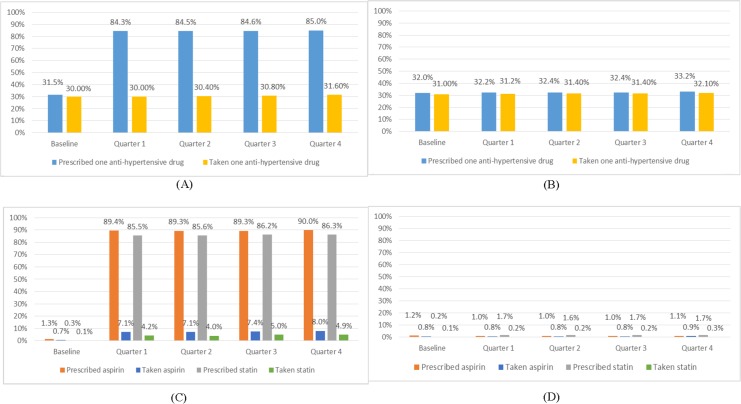
Results: A total of 28,130 participants, in 33 intervention and 34 control township hospitals, were recruited. Compared with the control arm, participants in the intervention arm had substantially improved prescribing rates of anti-hypertensives, statins and aspirin (P<0.001), and had higher medication taking rates of aspirin and statins (P<0.001). Mean systolic and diastolic blood pressures were similar across both arms (0.15 mmHg, P = 0.79, and 0.52 mmHg, P = 0.05, respectively). In the panel, (950) rates of smoking (OR = 0.23, P = 0.02) and salt intake (OR = 2.85, P = 0.03) were significantly reduced in the intervention versus control arms, but there were no statistically significant improvement over the 12 month follow-up period in biomedical indicators (P>0.05).
Conclusion: Implementation of the package by family doctors was feasible and improved prescribing and some lifestyle changes. Additional measures such as reducing medication costs and patient education are required.
Trial registration: Current Controlled Trials ISRCTN58988083.
Conflict of interest statement
Figures


References
-
- Uthman OA, Hartley L, Rees K, Taylor F, Ebrahim S, Clarke A. Multiple risk factor interventions for primary prevention of cardiovascular disease in low- and middle-income countries. The Cochrane database of systematic reviews. 2015;8:Cd011163 Epub 2015/08/15. doi: 10.1002/14651858.CD011163.pub2 . - DOI - PMC - PubMed
-
- Hypertension: uncontrolled and conquering the world. Lancet. 2007;370(9587):539 Epub 2007/08/21. doi: 10.1016/S0140-6736(07)61265-3 . - DOI - PubMed
-
- International Diabetes Federation. IDF Diabetes atlas Brussels: International Diabetes Federation; 2015 [cited 2015 November 10]. Available from: http://www.idf.org/diabetesatlas/.
-
- Norheim OF, Jha P, Admasu K, Godal T, Hum RJ, Kruk ME, et al. Avoiding 40% of the premature deaths in each country, 2010–30: review of national mortality trends to help quantify the UN Sustainable Development Goal for health. The Lancet. 385(9964):239–52. doi: 10.1016/S0140-6736(14)61591-9 - DOI - PubMed
-
- Chow CK, Teo KK, Rangarajan S, Islam S, Gupta R, Avezum A, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. Jama. 2013;310(9):959–68. doi: 10.1001/jama.2013.184182 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
