

Novel remote electronic medication supply model for opioid-dependent outpatients with polypharmacy--first long-term case study
- PMID: 28814330
- PMCID: PMC5559800
- DOI: 10.1186/s12954-017-0182-x
Novel remote electronic medication supply model for opioid-dependent outpatients with polypharmacy--first long-term case study
Abstract
Background: Patients with substance use disorders grow older thanks to effective treatments. Together with a high prevalence of comorbidities, psychological problems, and low social support, these patients are at high risk for medication non-adherence. Established treatment facilities face challenges to accommodate these complex patients within their setting. Electronic medication management aids (e-MMAs) might be appropriate to simultaneously monitor and improve adherence for these patients.
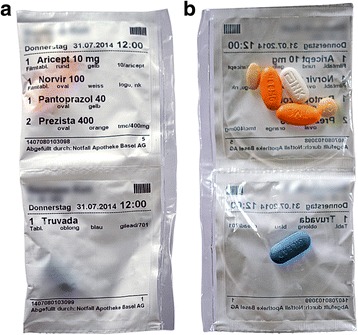
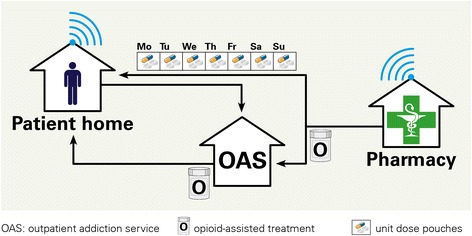
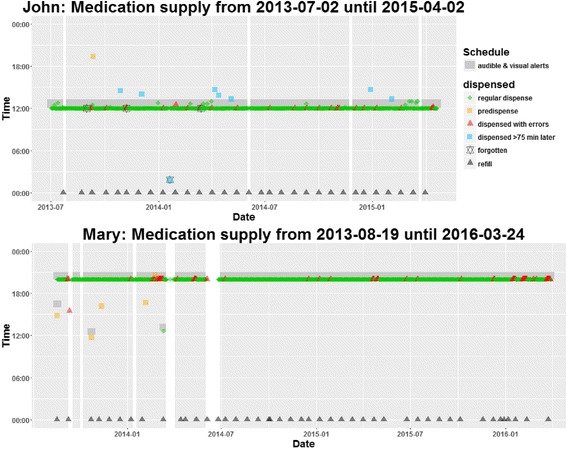
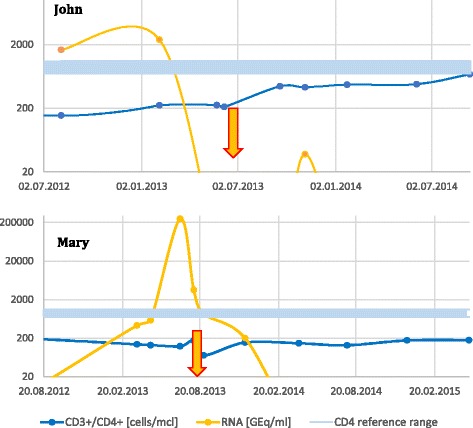
Case presentation: We report the first long-term experiences with a novel remote electronic medication supply model for two opioid-dependent patients with HIV. John (beginning dementia, 52 years, 6 tablets daily at 12 am) and Mary (frequent drug holidays, 48 years, 5-6 tablets daily at 8 pm) suffered from disease progression due to non-adherence. We electronically monitored adherence and clinical outcomes during 659 (John) and 953 (Mary) days between July 2013 and April 2016. Both patients retrieved over 90% of the pouches within 75 min of the scheduled time. Technical problems occurred in 4% (John) and 7.2% (Mary) of retrievals, but on-site support was seldom required. Viral loads fell below detection limits during the entire observation period.
Conclusions: Continuous medication supply and persistence with treatment of over 1.7 years, timing adherence of more than 90%, and suppressed HIV viral load are first results supporting the feasibility of the novel supply model for patients on opioid-assisted treatment and polypharmacy.
Keywords: Interprofessional collaboration; Medication adherence; Medication management aid; Old age; Substance use disorders.
Conflict of interest statement
Consent for publication
Informed consent was obtained from the patients for the publication of this case study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- European Monitoring Centre for Drugs and Drug Addiction . Treatment and care for older drug users. Luxembourg: Publications Office of the European Union; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
