

A modified efficient purse-string stapling technique (mEST) that uses a new metal rod for intracorporeal esophagojejunostomy in laparoscopic total gastrectomy
- PMID: 28815221
- PMCID: PMC5539391
- DOI: 10.21037/tgh.2017.06.01
A modified efficient purse-string stapling technique (mEST) that uses a new metal rod for intracorporeal esophagojejunostomy in laparoscopic total gastrectomy
Abstract
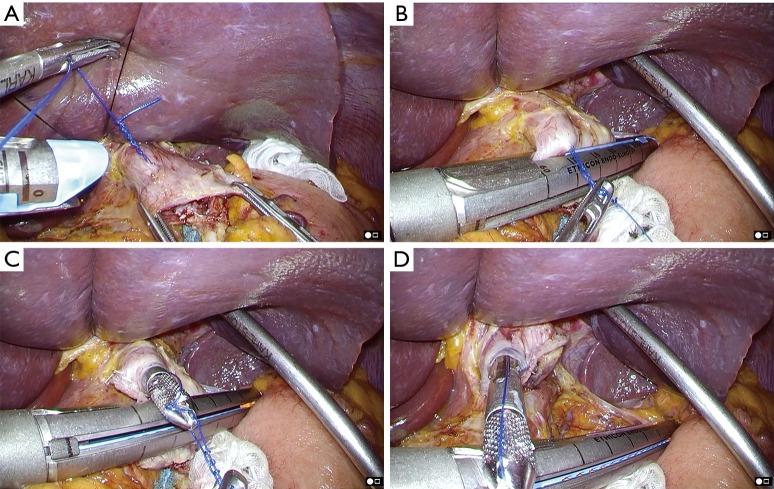
Intracorporeal esophagojejunostomy after laparoscopic total gastrectomy is technically difficult because this procedure should be performed in a narrow surgical field in the upper abdomen even when completely laparoscopic approaches are used. The placement of the anvil of a circular stapling device into the esophagus and connection the instrument to the anvil are extremely difficult steps in this surgery. Therefore, we developed a simple technique for intracorporeal esophagojejunostomy using hemi-double stapling technique; we named this technique the efficient purse-string stapling technique (EST). More recently, we have developed a modified EST (mEST) that utilizes a new stainless steel anvil rod instead of a plastic rod. Relative to the plastic rod, the steel rod is reusable and shorter; thus, it was easier to perform anvil placement into the esophagus with the steel rod. Anvil preparation for mEST: a stainless steel rod is attached to the shaft of the anvil, and the needle and thread are sutured to the tip of the rod. After complete insertion of the anvil into the esophageal cavity, the needle and thread are used to penetrate the anterior esophageal wall, and the esophagus is then clamped using a linear stapler just distal to the site penetrated by the thread. The linear stapler is fired, and anvil placement in the esophagus is simultaneously accomplished. After the rod is removed from the anvil, the instrument is intracorporeally connected to the anvil and then fired to complete the gastrojejunostomy. This technique is simple and facilitates intracorporeal reconstruction procedures in laparoscopic total gastrectomy.
Keywords: Laparoscopic total gastrectomy; circular stapling device; efficient purse-string stapling technique (EST); gastric cancer; hemi-double stapling technique.
Conflict of interest statement
Conflicts of Interest: The authors haves no conflicts of interest to declare.
Figures








References
-
- Kitano S, Iso Y, Moriyama M, et al. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 1994;4:146-8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials