

New astroglial injury-defined biomarkers for neurotrauma assessment
- PMID: 28816095
- PMCID: PMC5624401
- DOI: 10.1177/0271678X17724681
New astroglial injury-defined biomarkers for neurotrauma assessment
Abstract
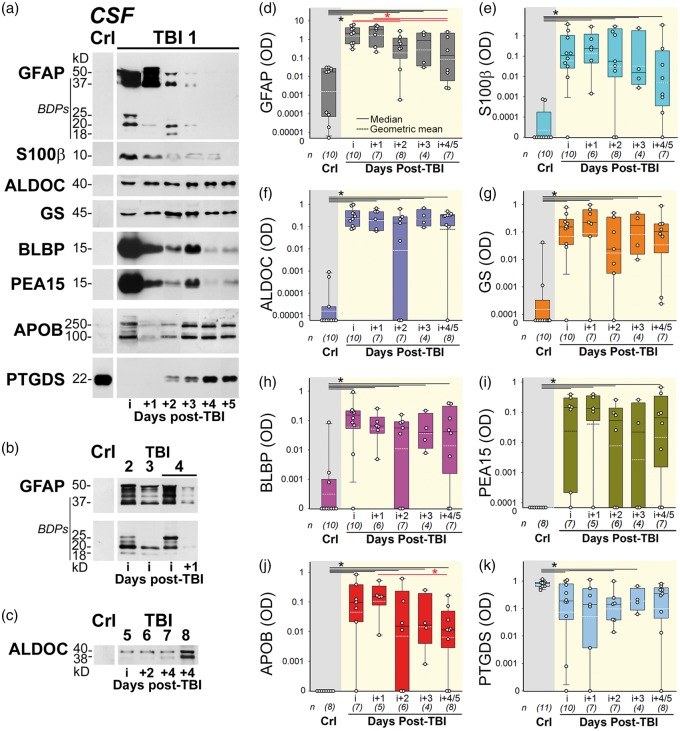
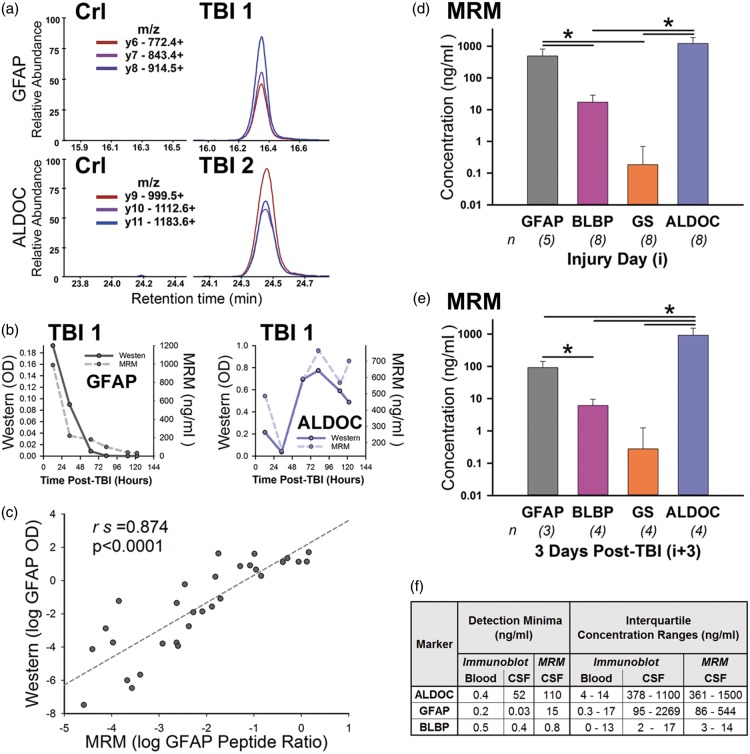
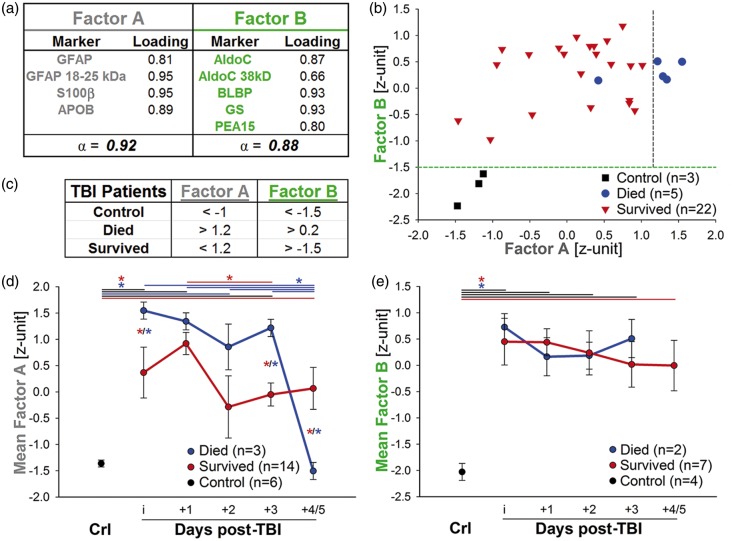
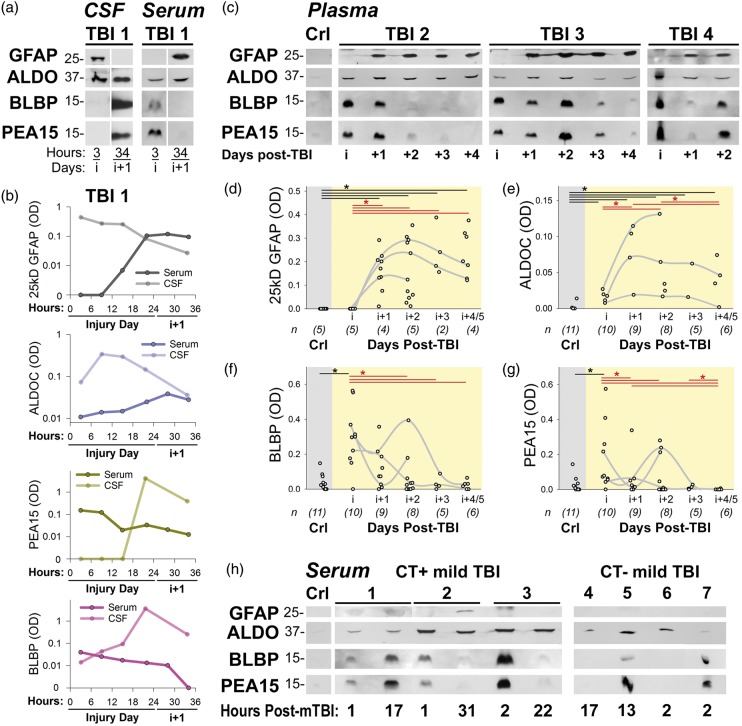
Traumatic brain injury (TBI) is an expanding public health epidemic with pathophysiology that is difficult to diagnose and thus treat. TBI biomarkers should assess patients across severities and reveal pathophysiology, but currently, their kinetics and specificity are unclear. No single ideal TBI biomarker exists. We identified new candidates from a TBI CSF proteome by selecting trauma-released, astrocyte-enriched proteins including aldolase C (ALDOC), its 38kD breakdown product (BDP), brain lipid binding protein (BLBP), astrocytic phosphoprotein (PEA15), glutamine synthetase (GS) and new 18-25kD-GFAP-BDPs. Their levels increased over four orders of magnitude in severe TBI CSF. First post-injury week, ALDOC levels were markedly high and stable. Short-lived BLBP and PEA15 related to injury progression. ALDOC, BLBP and PEA15 appeared hyper-acutely and were similarly robust in severe and mild TBI blood; 25kD-GFAP-BDP appeared overnight after TBI and was rarely present after mild TBI. Using a human culture trauma model, we investigated biomarker kinetics. Wounded (mechanoporated) astrocytes released ALDOC, BLBP and PEA15 acutely. Delayed cell death corresponded with GFAP release and proteolysis into small GFAP-BDPs. Associating biomarkers with cellular injury stages produced astroglial injury-defined (AID) biomarkers that facilitate TBI assessment, as neurological deficits are rooted not only in death of CNS cells, but also in their functional compromise.
Keywords: Astrocytes; brain trauma; cell culture; cerebrospinal fluid; exploratory factor analysis; proteomics.
Figures
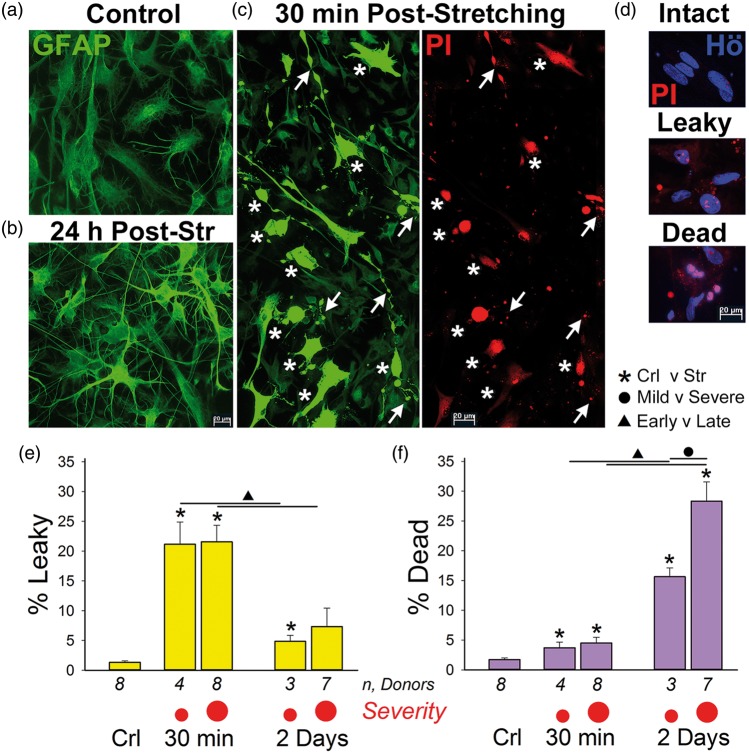
 , small red dot) and severe (4.4–5.3 PSI, large red dot, , p < 0.001) stretching. Leaky-cell fractions decreased between 30 min and 2d post injury (Δ, p < 0.01). (f) Median cell death numbers were slightly elevated at 30 min (*p < 0.05, mild; *p < 0.01 severe). Cell death substantially increased by 2d after stretching from 30 min (Δ, p < 0.0001, 2d difference to unstretched were *p < 0.01, mild; *p < 0.001, severe). A severity difference in cell death means was found at 2d post injury between mild and severely stretched cultures (indicated by a black dot • p < 0.001).
, small red dot) and severe (4.4–5.3 PSI, large red dot, , p < 0.001) stretching. Leaky-cell fractions decreased between 30 min and 2d post injury (Δ, p < 0.01). (f) Median cell death numbers were slightly elevated at 30 min (*p < 0.05, mild; *p < 0.01 severe). Cell death substantially increased by 2d after stretching from 30 min (Δ, p < 0.0001, 2d difference to unstretched were *p < 0.01, mild; *p < 0.001, severe). A severity difference in cell death means was found at 2d post injury between mild and severely stretched cultures (indicated by a black dot • p < 0.001).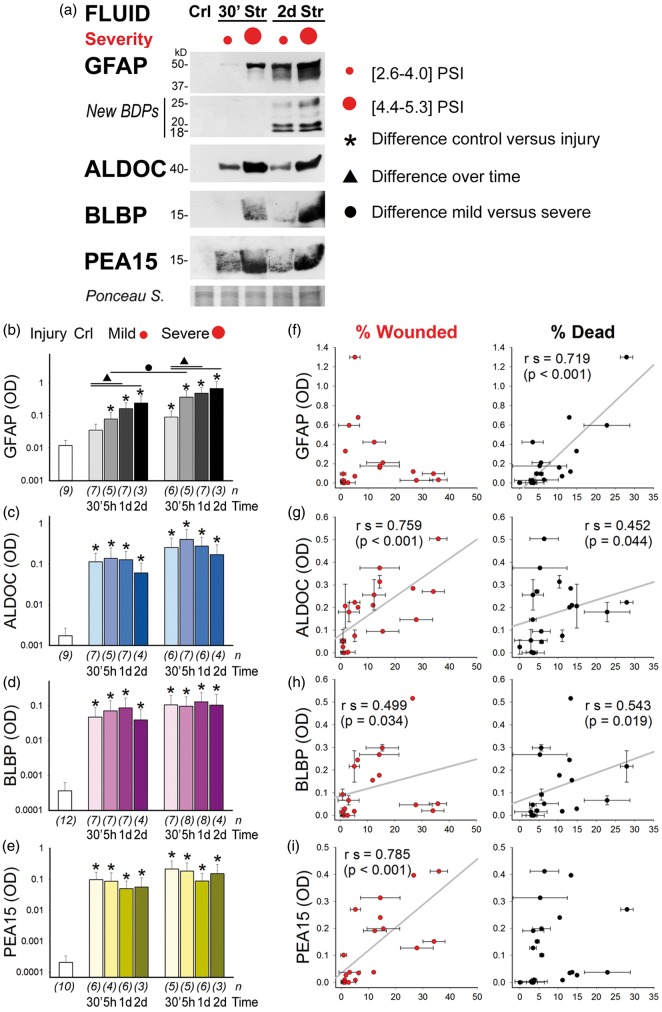 ) and severe stretched (4.4–5.3 psi, large red dot, ) astrocyte cultures are shown at 30 min (30′) and 2d post injury. Blots show fluid signals for GFAP, ALDOC, BLBP and PEA15. Small GFAP-BDPs (25–18 kD) were absent at 30 min and present by 2d post injury, whereas ALDOC, BLBP and PEA15 were present 30 min post injury and at 2d. Ponceau S shows total protein amount for 30 µl fluid per lane. (b–e) Geometric means of optical densities (OD) for (b) GFAP, (c) ALDOC, (d) BLBP and (e) PEA15 are plotted for unstretched, 30 min, 5 h, 1d and 2d mild and severe stretched cultures. All stretched fluid samples show significant biomarker elevation compared to those of unstretched fluids (*GFAP 5 h mild stretch: p = 0.005, all others p < 0.001; n = number of donors). The exception was that GFAP elevation in fluids was only threefold (p > 0.05) 30 min after mild stretching. In contrast, 30-min mild stretched cultures had significantly elevated levels of ALDOC (66-fold), BLBP (130-fold), and PEA15 (460-fold, all *p < 0.001). GFAP release levels increased over indicated times (see lines and ▴, p < 0.02). GFAP levels showed severity difference at 5 h after stretching (•, p = 0.042). Severity differences for ALDOC, BLBP and PEA15 were two-threefold and not significant. (f–i) Biplots correlate biomarker levels on y-axes with percent wounded astrocytes (red, leaky) and percent dead cells (black) on x-axes. Spearman correlations (rs) are given with p-values and lines of best fit. Error bars are standard deviations of replicate analyses. (f) GFAP correlated only with cell death rates. (g) ALDOC and (h) BLBP correlated with cell wounding and cell death. (i) PEA15 correlated only with cell wounding.
) and severe stretched (4.4–5.3 psi, large red dot, ) astrocyte cultures are shown at 30 min (30′) and 2d post injury. Blots show fluid signals for GFAP, ALDOC, BLBP and PEA15. Small GFAP-BDPs (25–18 kD) were absent at 30 min and present by 2d post injury, whereas ALDOC, BLBP and PEA15 were present 30 min post injury and at 2d. Ponceau S shows total protein amount for 30 µl fluid per lane. (b–e) Geometric means of optical densities (OD) for (b) GFAP, (c) ALDOC, (d) BLBP and (e) PEA15 are plotted for unstretched, 30 min, 5 h, 1d and 2d mild and severe stretched cultures. All stretched fluid samples show significant biomarker elevation compared to those of unstretched fluids (*GFAP 5 h mild stretch: p = 0.005, all others p < 0.001; n = number of donors). The exception was that GFAP elevation in fluids was only threefold (p > 0.05) 30 min after mild stretching. In contrast, 30-min mild stretched cultures had significantly elevated levels of ALDOC (66-fold), BLBP (130-fold), and PEA15 (460-fold, all *p < 0.001). GFAP release levels increased over indicated times (see lines and ▴, p < 0.02). GFAP levels showed severity difference at 5 h after stretching (•, p = 0.042). Severity differences for ALDOC, BLBP and PEA15 were two-threefold and not significant. (f–i) Biplots correlate biomarker levels on y-axes with percent wounded astrocytes (red, leaky) and percent dead cells (black) on x-axes. Spearman correlations (rs) are given with p-values and lines of best fit. Error bars are standard deviations of replicate analyses. (f) GFAP correlated only with cell death rates. (g) ALDOC and (h) BLBP correlated with cell wounding and cell death. (i) PEA15 correlated only with cell wounding.
References
-
- Roozenbeek B, Maas AI, Menon DK. Changing patterns in the epidemiology of traumatic brain injury. Nat Rev Neurol 2013; 9: 231–236. - PubMed
-
- Rosenbaum SB, Lipton ML. Embracing chaos: the scope and importance of clinical and pathological heterogeneity in mTBI. Brain Imag Behav 2012; 6: 255–282. - PubMed
-
- Buki A, Kovacs N, Czeiter E, et al. Minor and repetitive head injury. Adv Tech Stand Neurosurg 2015; 42: 147–192. - PubMed
-
- Helmick KM, Spells CA, Malik SZ, et al. Traumatic brain injury in the US military: epidemiology and key clinical and research programs. Brain Imag Behav 2015; 9: 358–366. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
