

Phase I/II Trial of Labetuzumab Govitecan (Anti-CEACAM5/SN-38 Antibody-Drug Conjugate) in Patients With Refractory or Relapsing Metastatic Colorectal Cancer
- PMID: 28817371
- PMCID: PMC8259133
- DOI: 10.1200/JCO.2017.73.9011
Phase I/II Trial of Labetuzumab Govitecan (Anti-CEACAM5/SN-38 Antibody-Drug Conjugate) in Patients With Refractory or Relapsing Metastatic Colorectal Cancer
Abstract
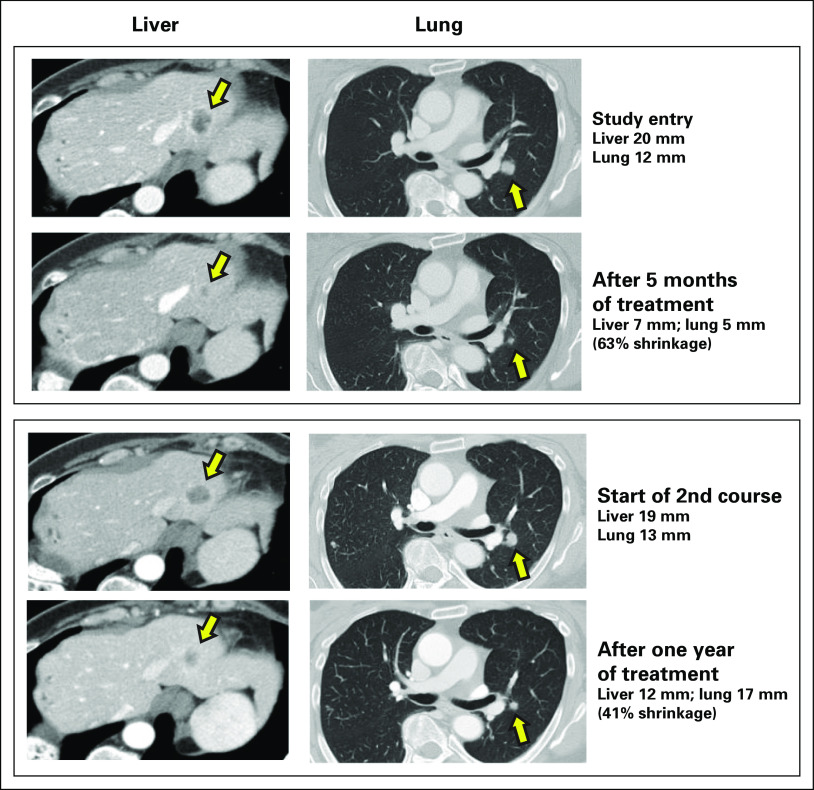
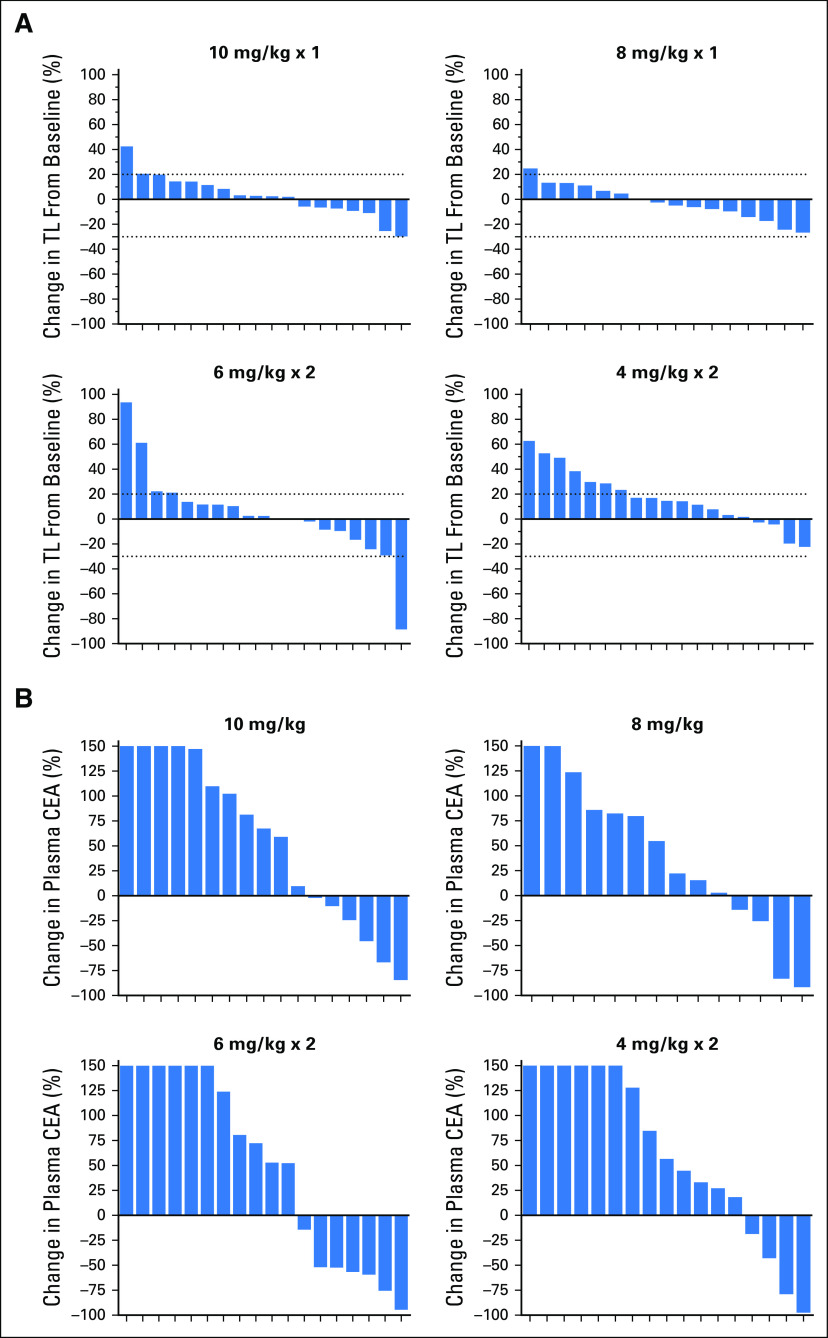
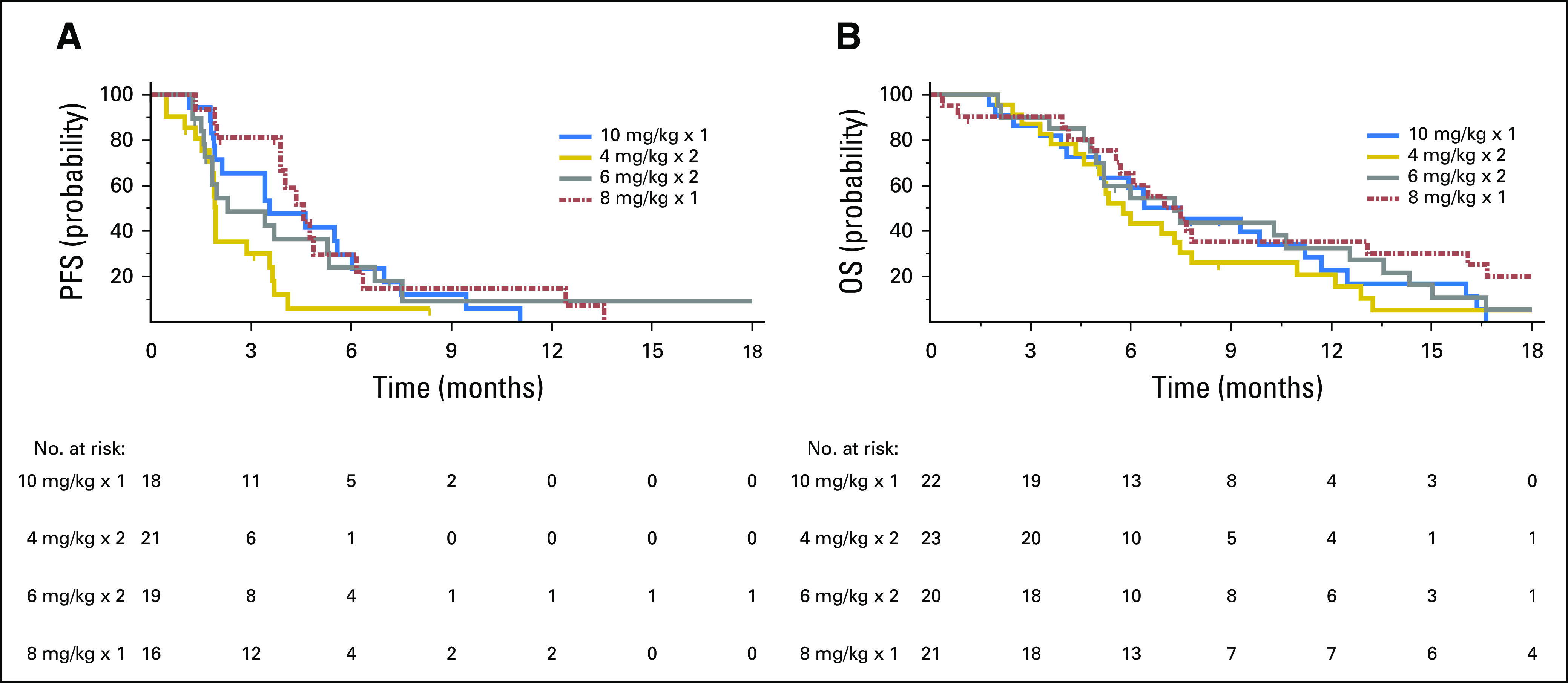
Purpose The objectives were to evaluate dosing schedules of labetuzumab govitecan, an antibody-drug conjugate targeting carcinoembryonic antigen-related cell adhesion molecule 5 (CEACAM5) for tumor delivery of 7-ethyl-10-hydroxycamptothecin (SN-38), in an expanded phase II trial of patients with relapsed or refractory metastatic colorectal cancer. Patients and Methods Eligible patients with at least one prior irinotecan-containing therapy received labetuzumab govitecan once weekly at 8 and 10 mg/kg, or two times per week at 4 and 6 mg/km on weeks 1 and 2 of 3-week repeated cycles. End points were safety, response, pharmacokinetics, and immunogenicity. Results Eighty-six patients who had undergone a median of five prior therapies (range, one to 13) were each enrolled into one of the four cohorts. On the basis of Response Evaluation Criteria in Solid Tumors 1.1, 38% of these patients had a tumor as well as plasma carcinoembryonic antigen reduction from baseline after labetuzumab govitecan treatment; one patient achieved a partial response with a sustained response spanning > 2 years, whereas 42 patients had stable disease as the best overall response. Median progression-free survival and overall survival were 3.6 and 6.9 months, respectively. The major toxicities (grade ≥ 3) among all cohorts were neutropenia (16%), leukopenia (11%), anemia (9%), and diarrhea (7%). The antibody-drug conjugate's mean half-life was 16.5 hours for the four cohorts. Anti-drug/anti-antibody antibodies were not detected. The two once-weekly dose schedules, showing comparable toxicity and efficacy, were chosen for further study. Conclusion Monotherapy with labetuzumab govitecan demonstrated a manageable safety profile and therapeutic activity in heavily pretreated patients with metastatic colorectal cancer, all with prior irinotecan therapy. Further studies of labetuzumab govitecan treatment alone or in combination with other therapies in earlier settings are indicated.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA, et al: Colorectal cancer statistics, 2017. CA Cancer J Clin 67:177-193, 2017. - PubMed
-
- Siegel RL, Miller KD, Jemal A: Cancer Statistics, 2017. CA Cancer J Clin 67:7-30, 2017 - PubMed
-
- Van Cutsem E, Cervantes A, Nordlinger B, et al. : Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 25:iii1-iii9, 2014 - PubMed
-
- Bertocchi P, Aroldi F, Prochilo T, et al. : Chemotherapy rechallenge after regorafenib treatment in metastatic colorectal cancer: Still hope after the last hope? J Chemother 29:102-105, 2017 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
