

Incorporating Dynamic Assessment of Fluid Responsiveness Into Goal-Directed Therapy: A Systematic Review and Meta-Analysis
- PMID: 28817481
- PMCID: PMC5555977
- DOI: 10.1097/CCM.0000000000002554
Incorporating Dynamic Assessment of Fluid Responsiveness Into Goal-Directed Therapy: A Systematic Review and Meta-Analysis
Abstract
Objective: Dynamic tests of fluid responsiveness have been developed and investigated in clinical trials of goal-directed therapy. The impact of this approach on clinically relevant outcomes is unknown. We performed a systematic review and meta-analysis to evaluate whether fluid therapy guided by dynamic assessment of fluid responsiveness compared with standard care improves clinically relevant outcomes in adults admitted to the ICU.
Data sources: Randomized controlled trials from MEDLINE, EMBASE, CENTRAL, clinicaltrials.gov, and the International Clinical Trials Registry Platform from inception to December 2016, conference proceedings, and reference lists of relevant articles.
Study selection: Two reviewers independently identified randomized controlled trials comparing dynamic assessment of fluid responsiveness with standard care for acute volume resuscitation in adults admitted to the ICU.
Data extraction: Two reviewers independently abstracted trial-level data including population characteristics, interventions, clinical outcomes, and source of funding. Our primary outcome was mortality at longest duration of follow-up. Our secondary outcomes were ICU and hospital length of stay, duration of mechanical ventilation, and frequency of renal complications. The internal validity of trials was assessed in duplicate using the Cochrane Collaboration's Risk of Bias tool.
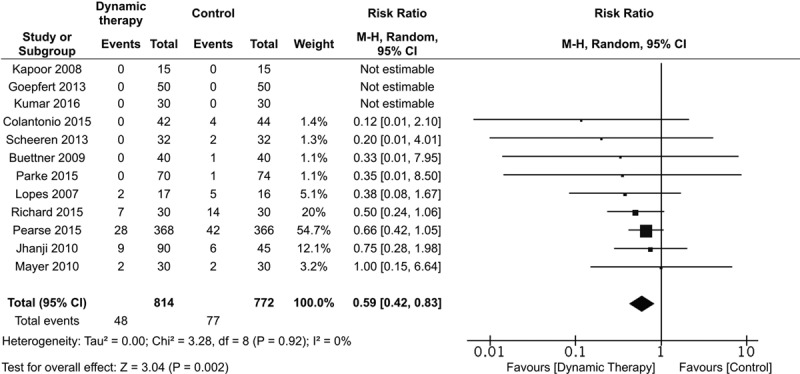
Data synthesis: We included 13 trials enrolling 1,652 patients. Methods used to assess fluid responsiveness included stroke volume variation (nine trials), pulse pressure variation (one trial), and stroke volume change with passive leg raise/fluid challenge (three trials). In 12 trials reporting mortality, the risk ratio for death associated with dynamic assessment of fluid responsiveness was 0.59 (95% CI, 0.42-0.83; I = 0%; n = 1,586). The absolute risk reduction in mortality associated with dynamic assessment of fluid responsiveness was -2.9% (95% CI, -5.6% to -0.2%). Dynamic assessment of fluid responsiveness was associated with reduced duration of ICU length of stay (weighted mean difference, -1.16 d [95% CI, -1.97 to -0.36]; I = 74%; n = 394, six trials) and mechanical ventilation (weighted mean difference, -2.98 hr [95% CI, -5.08 to -0.89]; I = 34%; n = 334, five trials). Three trials were adjudicated at unclear risk of bias; the remaining trials were at high risk of bias.
Conclusions: In adult patients admitted to intensive care who required acute volume resuscitation, goal-directed therapy guided by assessment of fluid responsiveness appears to be associated with reduced mortality, ICU length of stay, and duration of mechanical ventilation. High-quality clinical trials in both medical and surgical ICU populations are warranted to inform routine care.
Conflict of interest statement
Dr. Bednarczyk disclosed that Dr. Zarychanski receives salary support from the Canadian Institute of Health Research. Dr. Turgeon is the Canada Research Chair in Critical Care Neurology and Trauma. These entities have had no role in the design or conduct of the study or approval of the final report. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Marik P, Bellomo R. A rational approach to fluid therapy in sepsis. Br J Anaesth 2016; 116:339–349. - PubMed
-
- Kanji HD, McCallum J, Sirounis D, et al. Limited echocardiography-guided therapy in subacute shock is associated with change in management and improved outcomes. J Crit Care 2014; 29:700–705. - PubMed
-
- Boyd JH, Forbes J, Nakada TA, et al. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med 2011; 39:259–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
