

End-Tidal CO2-Guided Chest Compression Delivery Improves Survival in a Neonatal Asphyxial Cardiac Arrest Model
- PMID: 28817508
- PMCID: PMC5669831
- DOI: 10.1097/PCC.0000000000001299
End-Tidal CO2-Guided Chest Compression Delivery Improves Survival in a Neonatal Asphyxial Cardiac Arrest Model
Abstract
Objectives: To determine whether end-tidal CO2-guided chest compression delivery improves survival over standard cardiopulmonary resuscitation after prolonged asphyxial arrest.
Design: Preclinical randomized controlled study.
Setting: University animal research laboratory.
Subjects: 1-2-week-old swine.
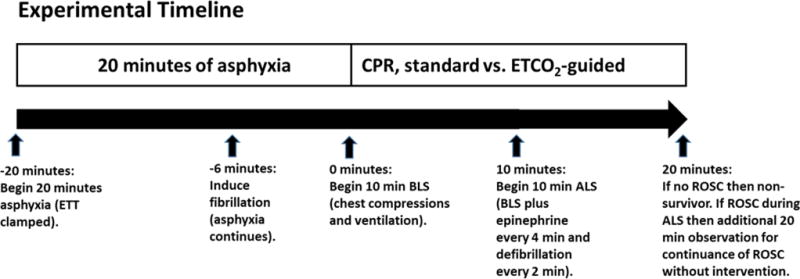
Interventions: After undergoing a 20-minute asphyxial arrest, animals received either standard or end-tidal CO2-guided cardiopulmonary resuscitation. In the standard group, chest compression delivery was optimized by video and verbal feedback to maintain the rate, depth, and release within published guidelines. In the end-tidal CO2-guided group, chest compression rate and depth were adjusted to obtain a maximal end-tidal CO2 level without other feedback. Cardiopulmonary resuscitation included 10 minutes of basic life support followed by advanced life support for 10 minutes or until return of spontaneous circulation.
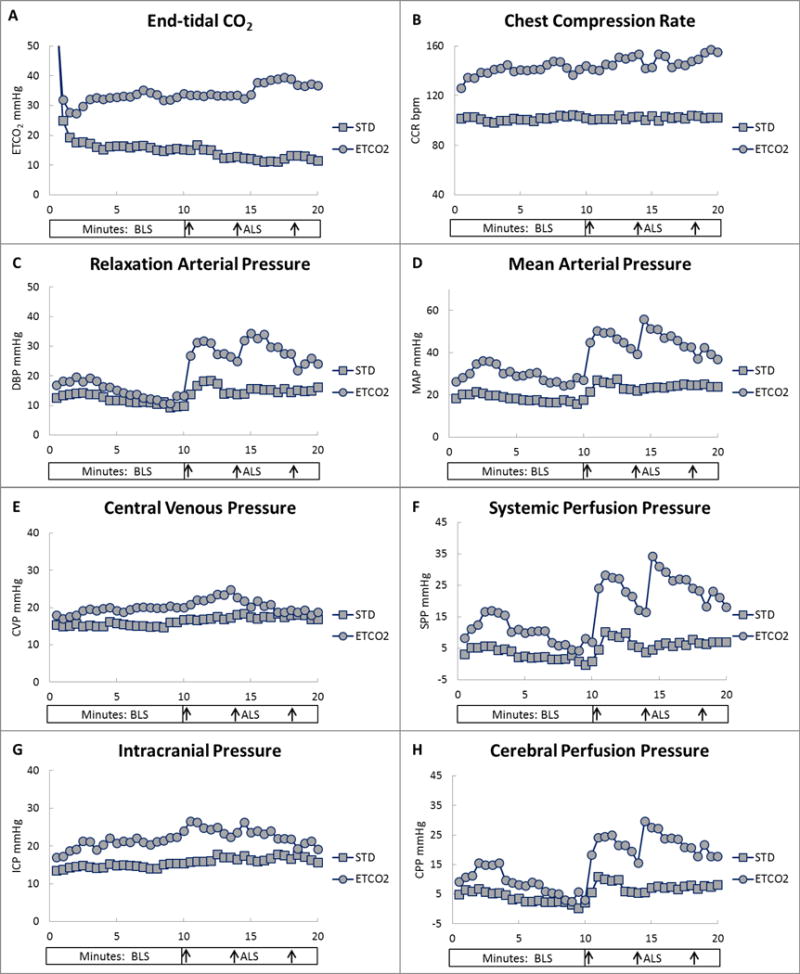
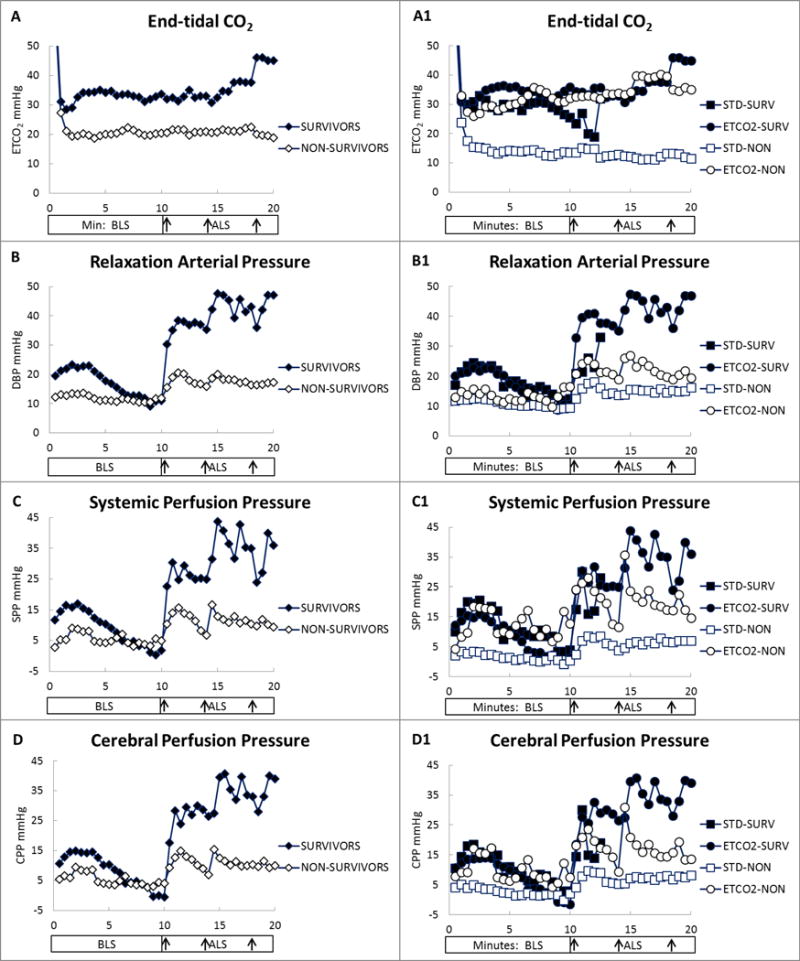
Measurements and main results: Mean end-tidal CO2 at 10 minutes of cardiopulmonary resuscitation was 34 ± 8 torr in the end-tidal CO2 group (n = 14) and 19 ± 9 torr in the standard group (n = 14; p = 0.0001). The return of spontaneous circulation rate was 7 of 14 (50%) in the end-tidal CO2 group and 2 of 14 (14%) in the standard group (p = 0.04). The chest compression rate averaged 143 ± 10/min in the end-tidal CO2 group and 102 ± 2/min in the standard group (p < 0.0001). Neither asphyxia-related hypercarbia nor epinephrine administration confounded the use of end-tidal CO2-guided chest compression delivery. The response of the relaxation arterial pressure and cerebral perfusion pressure to the initial epinephrine administration was greater in the end-tidal CO2 group than in the standard group (p = 0.01 and p = 0.03, respectively). The prevalence of resuscitation-related injuries was similar between groups.
Conclusions: End-tidal CO2-guided chest compression delivery is an effective resuscitation method that improves early survival after prolonged asphyxial arrest in this neonatal piglet model. Optimizing end-tidal CO2 levels during cardiopulmonary resuscitation required that chest compression delivery rate exceed current guidelines. The use of physiologic feedback during cardiopulmonary resuscitation has the potential to provide optimized and individualized resuscitative efforts.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
The Future of Resuscitation: Personalized Physiology-Guided Cardiopulmonary Resuscitation.Pediatr Crit Care Med. 2017 Nov;18(11):1084-1086. doi: 10.1097/PCC.0000000000001316. Pediatr Crit Care Med. 2017. PMID: 29099457 No abstract available.
References
-
- Kleinman ME, Chameides L, Schexnayder SM, et al. Pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics. 2010;126:e1361–e1399. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
