

Peripheral clinic versus centralized laboratory-based Xpert MTB/RIF performance: Experience gained from a pragmatic, stepped-wedge trial in Botswana
- PMID: 28817643
- PMCID: PMC5560557
- DOI: 10.1371/journal.pone.0183237
Peripheral clinic versus centralized laboratory-based Xpert MTB/RIF performance: Experience gained from a pragmatic, stepped-wedge trial in Botswana
Abstract
Background: In 2011, the Botswana National Tuberculosis Program adopted World Health Organization guidelines and introduced Xpert MTB/RIF (Xpert) assay to support intensified case finding among people living with HIV enrolling in care. An evaluation was designed to assess performance under operational conditions to inform the national Xpert scale-up.
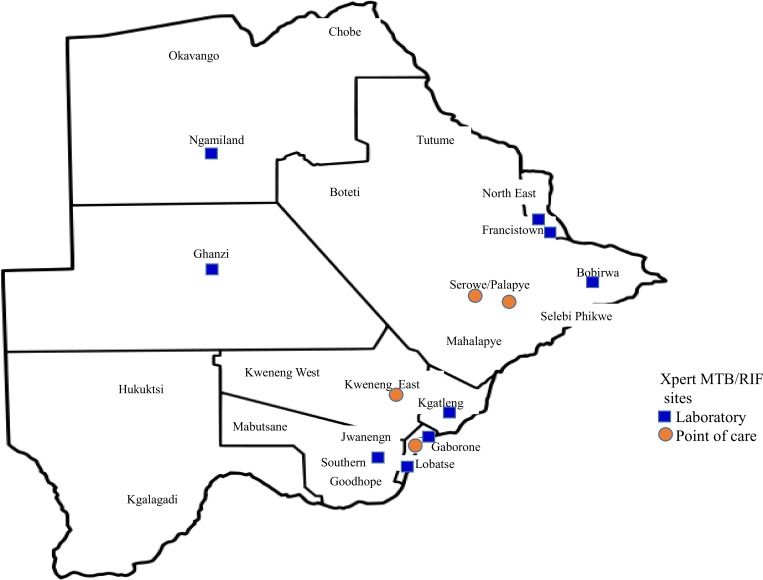
Methods: Xpert was implemented from August 2012 through November 2014 with 13 GeneXpert instruments (GeneXpert) deployed in a phased approach over nine months: nine centralized laboratory and four point-of-care (POC) peripheral clinics. Clinicians and laboratorians were trained on the four-symptom tuberculosis screening algorithm and Xpert testing. We documented our experience with staff training and GeneXpert performance. Test results were extracted from GeneXpert software; unsuccessful tests were analysed in relation to testing sites and trends over time.
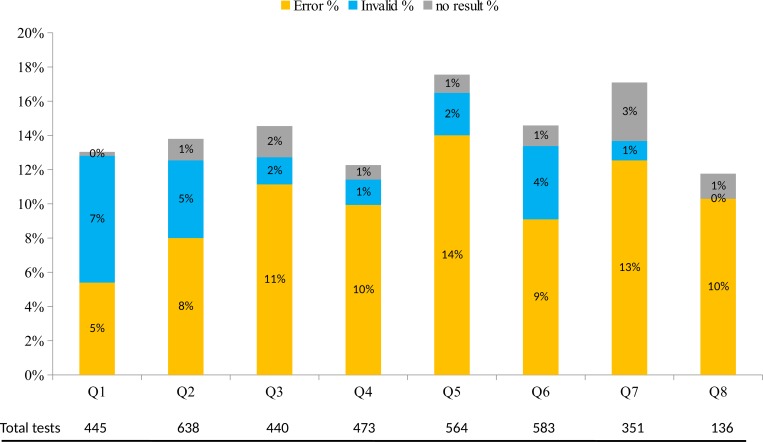
Results: During 276 instrument-months of operation a total of 3,630 tests were performed, of which 3,102 (85%) were successful with interpretable results. Mycobacterium tuberculosis complex was detected for 447 (14%); of these, 36 (8%) were rifampicin resistant. Of all 3,630 Xpert tests, 528 (15%) were unsuccessful; of these 361 (68%) were classified as "error", 119 (23%) as "invalid" and 48 (9%) as "no result". The total number of recorded error codes was 385 and the most common reasons were related to sample processing (211; 55%) followed by power supply (77; 20%) and cartridge/module related (54; 14%). Cumulative incidence of unsuccessful test was similar between POC (17%, 95% CI: 11-25%) and centralized laboratory-based GeneXpert instruments (14%, 95% CI: 11-17%; p = 0.140).
Conclusions: Xpert introduction was successful in the Botswana setting. The incidence of unsuccessful test was similar by GeneXpert location (POC vs. centralized laboratory). However, unsuccessful test incidence (15%) in our settings was higher than previously reported and was mostly related to improper sample processing. Ensuring adequate training among Xpert testing staff is essential to minimize errors.
Conflict of interest statement
Figures
References
-
- World Health Organization., Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children: Policy update WHO. 2013. Avaiable from: http://apps.who.int/iris/bitstream/10665/112472/1/9789241506335_eng.pdf - PubMed
-
- Botswana Aids Impact Survey IV report. Botswana 2013.
-
- Ansari N, Kombe A, Kenyon T, Hone N, Tappero J, Nyirenda S, et al. Pathology and causes of death in a group of 128 predominantly HIV-positive patients in Botswana, 1997–1998. Int J Tuberc Lung Dis. 2002; 6(1): 55–63. - PubMed
-
- Gupta R, Lucas S, Fielding K, Lawn S. Prevalence of tuberculosis in post-mortem studies of HIV-infected adults and children in resource-limited settings: a systematic review and meta-analysis. AIDS 2015, 29:1987–2002. doi: 10.1097/QAD.0000000000000802 - DOI - PMC - PubMed
-
- World Health Organization., Global tuberculosis report. WHO/HTM/TB/2015.22. Geneva: WHO. 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
