

Investigation of the halo-artifact in 68Ga-PSMA-11-PET/MRI
- PMID: 28817656
- PMCID: PMC5560715
- DOI: 10.1371/journal.pone.0183329
Investigation of the halo-artifact in 68Ga-PSMA-11-PET/MRI
Abstract
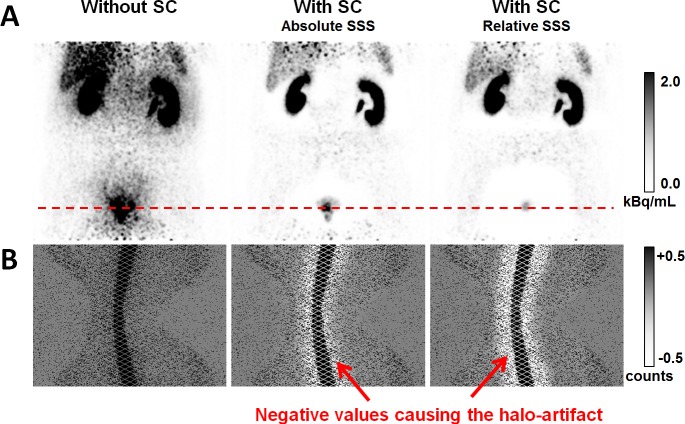
Objectives: Combined positron emission tomography (PET) and magnetic resonance imaging (MRI) targeting the prostate-specific membrane antigen (PSMA) with a 68Ga-labelled PSMA-analog (68Ga-PSMA-11) is discussed as a promising diagnostic method for patients with suspicion or history of prostate cancer. One potential drawback of this method are severe photopenic (halo-) artifacts surrounding the bladder and the kidneys in the scatter-corrected PET images, which have been reported to occur frequently in clinical practice. The goal of this work was to investigate the occurrence and impact of these artifacts and, secondly, to evaluate variants of the standard scatter correction method with regard to halo-artifact suppression.
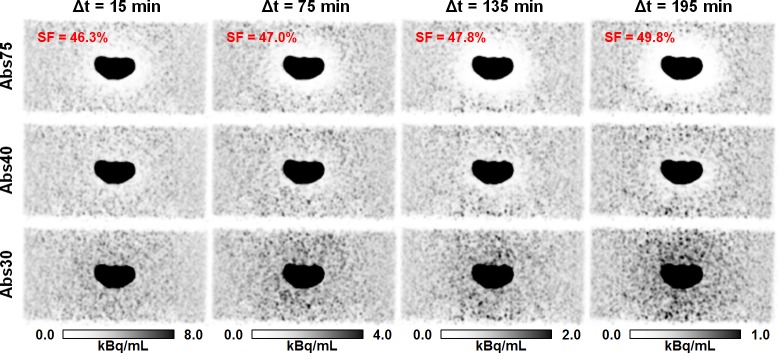
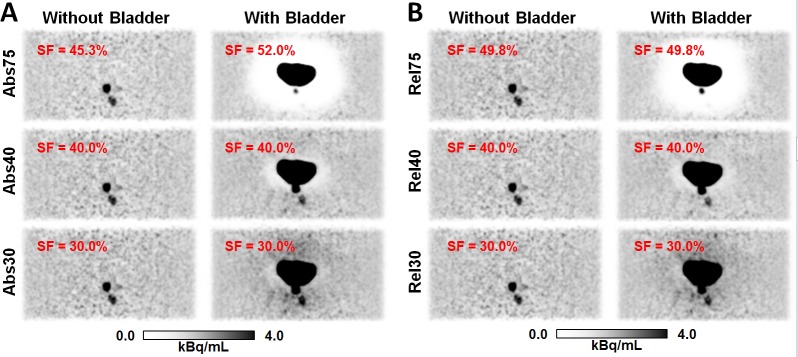
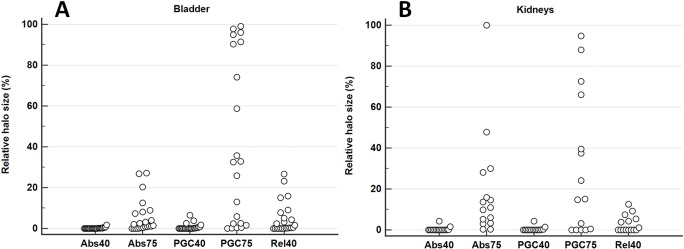
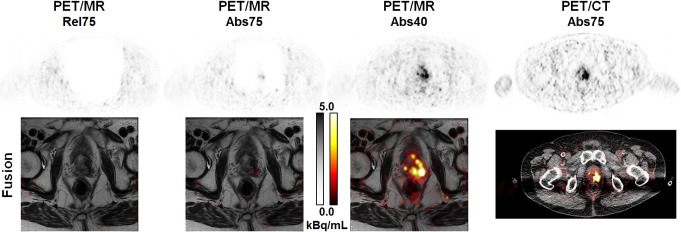
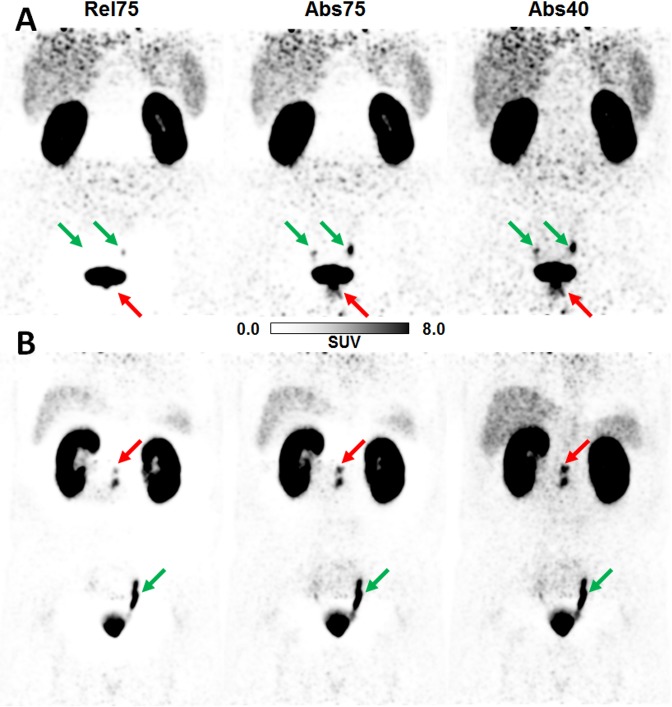
Methods: Experiments using a dedicated pelvis phantom were conducted to investigate whether the halo-artifact is modality-, tracer-, and/or concentration-dependent. Furthermore, 31 patients with history of prostate cancer were selected from an ongoing 68Ga-PSMA-11-PET/MRI study. For each patient, PET raw data were reconstructed employing six different variants of PET scatter correction: absolute scatter scaling, relative scatter scaling, and relative scatter scaling combined with prompt gamma correction, each of which was combined with a maximum scatter fraction (MaxSF) of MaxSF = 75% or MaxSF = 40%. Evaluation of the reconstructed images with regard to halo-artifact suppression was performed both quantitatively using statistical analysis and qualitatively by two independent readers.
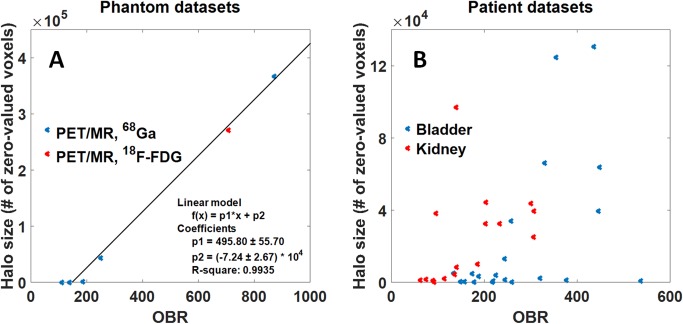
Results: The phantom experiments did not reveal any modality-dependency (PET/MRI vs. PET/CT) or tracer-dependency (68Ga vs. 18F-FDG). Patient- and phantom-based data indicated that halo-artifacts derive from high organ-to-background activity ratios (OBR) between bladder/kidneys and surrounding soft tissue, with a positive correlation between OBR and halo size. Comparing different variants of scatter correction, reducing the maximum scatter fraction from the default value MaxSF = 75% to MaxSF = 40% was found to efficiently suppress halo-artifacts in both phantom and patient data. In 1 of 31 patients, reducing the maximum scatter fraction provided new PET-based information changing the patient's diagnosis.
Conclusion: Halo-artifacts are particularly observed for 68Ga-PSMA-11-PET/MRI due to 1) the biodistribution of the PSMA-11-tracer resulting in large OBRs for bladder and kidneys and 2) inaccurate scatter correction methods currently used in clinical routine, which tend to overestimate the scatter contribution. If not compensated for, 68Ga-PSMA-11 uptake pathologies may be masked by halo-artifacts leading to false-negative diagnoses. Reducing the maximum scatter fraction was found to efficiently suppress halo-artifacts.
Conflict of interest statement
Figures


References
-
- Silver DA, Pellicer I, Fair WR, Heston WWD, Cordon-Cardo C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin Cancer Res. 1997;3:81–85. - PubMed
-
- Sweat SD, Pacelli A, Murphy GP, Bostwick DG. Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology. 1998;52:637–640. - PubMed
-
- Eder M, Eisenhut M, Babich J, Haberkorn U. PSMA as a target for radiolabelled small molecules. Eur J Nucl Med Mol Imaging. 2013;40:819–823. doi: 10.1007/s00259-013-2374-2 - DOI - PMC - PubMed
-
- Eder M, Schäfer M, Bauder-Wüst U, Hull W-E, Wängler C, Mier W, et al. 68Ga-complex lipophilicity and the targeting property of a urea-based PSMA inhibitor for PET imaging. Bioconjug Chem. 2012;23:688–697. doi: 10.1021/bc200279b - DOI - PubMed
-
- Afshar-Oromieh A, Malcher A, Eder M, Eisenhut M, Linhart HG, Hadaschik BA, et al. PET imaging with a [68Ga]gallium-labelled PSMA ligand for the diagnosis of prostate cancer: biodistribution in humans and first evaluation of tumour lesions. Eur J Nucl Med Mol Imaging. 2013;40:486–495. doi: 10.1007/s00259-012-2298-2 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
