

Completeness of malaria indicator data reporting via the District Health Information Software 2 in Kenya, 2011-2015
- PMID: 28818071
- PMCID: PMC5561621
- DOI: 10.1186/s12936-017-1973-y
Completeness of malaria indicator data reporting via the District Health Information Software 2 in Kenya, 2011-2015
Abstract
Background: Health facility-based data reported through routine health information systems form the primary data source for programmatic monitoring and evaluation in most developing countries. The adoption of District Health Information Software (DHIS2) has contributed to improved availability of routine health facility-based data in many low-income countries. An assessment of malaria indicators data reported by health facilities in Kenya during the first 5 years of implementation of DHIS2, from January 2011 to December 2015, was conducted.
Methods: Data on 19 malaria indicators reported monthly by health facilities were extracted from the online Kenya DHIS2 database. Completeness of reporting was analysed for each of the 19 malaria indicators and expressed as the percentage of data values actually reported over the expected number; all health facilities were expected to report data for each indicator for all 12 months in a year.
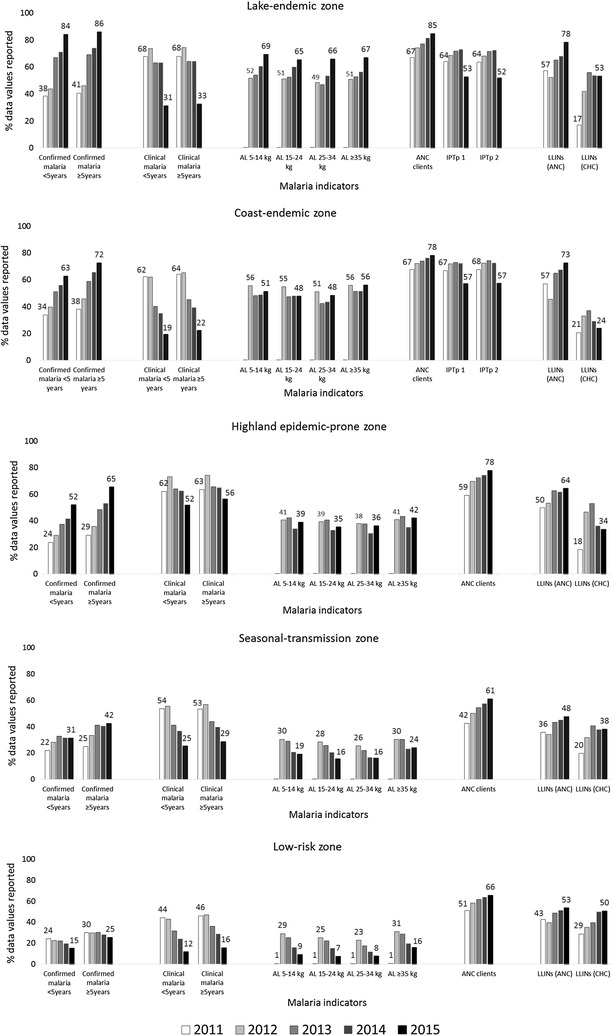
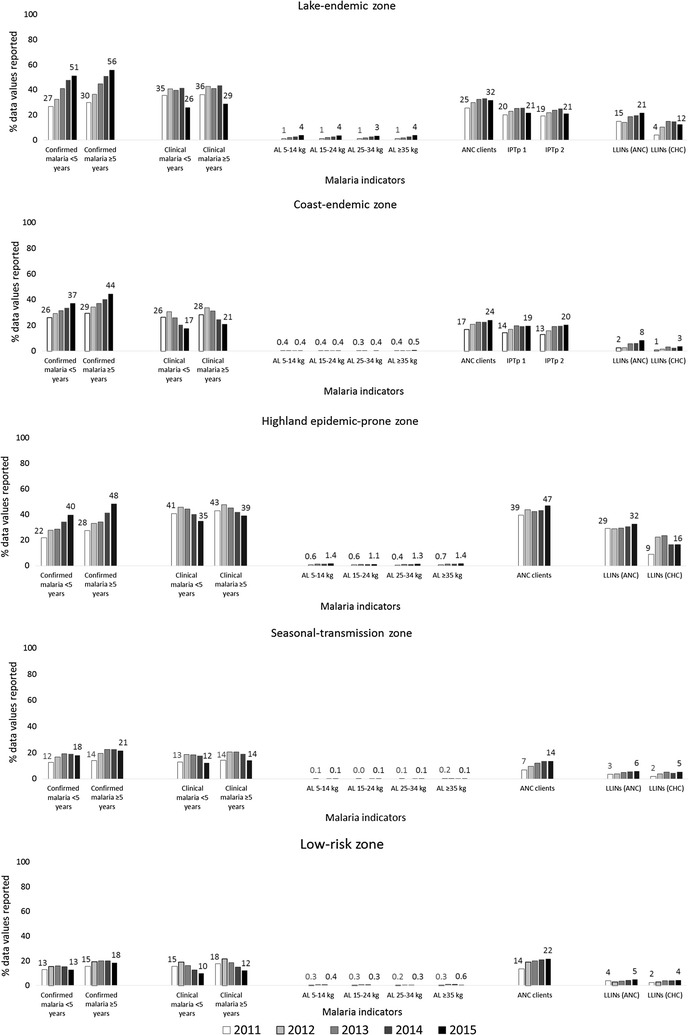
Results: Malaria indicators data were analysed for 6235 public and 3143 private health facilities. Between 2011 and 2015, completeness of reporting in the public sector increased significantly for confirmed malaria cases across all age categories (26.5-41.9%, p < 0.0001, in children aged <5 years; 30.6-51.4%, p < 0.0001, in persons aged ≥5 years). Completeness of reporting of new antenatal care (ANC) clients increased from 53.7 to 70.5%, p < 0.0001). Completeness of reporting of intermittent preventive treatment in pregnancy (IPTp) decreased from 64.8 to 53.7%, p < 0.0001 for dose 1 and from 64.6 to 53.4%, p < 0.0001 for dose 2. Data on malaria tests performed and test results were not available in DHIS2 from 2011 to 2014. In 2015, sparse data on microscopy (11.5% for children aged <5 years; 11.8% for persons aged ≥5 years) and malaria rapid diagnostic tests (RDTs) (8.1% for all ages) were reported. In the private sector, completeness of reporting increased significantly for confirmed malaria cases across all age categories (16.7-23.1%, p < 0.0001, in children aged <5 years; 19.4-28.6%, p < 0.0001, in persons aged ≥5 years). Completeness of reporting also improved for new ANC clients (16.2-23.6%, p < 0.0001), and for IPTp doses 1 and 2 (16.6-20.2%, p < 0.0001 and 15.5-20.5%, p < 0.0001, respectively). In 2015, less than 3% of data values for malaria tests performed were reported in DHIS2 from the private sector.
Conclusions: There have been sustained improvements in the completeness of data reported for most key malaria indicators since the adoption of DHIS2 in Kenya in 2011. However, major data gaps were identified for the malaria-test indicator and overall low reporting across all indicators from private health facilities. A package of proven DHIS2 implementation interventions and performance-based incentives should be considered to improve private-sector data reporting.
Figures
References
-
- WHO . Toolkit on monitoring health systems strengthening. Geneva: World Health Organization; 2008.
-
- WHO. Assessment of health facility data quality; data quality report card Uganda, 2010–2011. Geneva: World Health Organization; 2011.
-
- Nisingizwe MP, Iyer HS, Gashayija M, Hirschhorn LR, Amoroso C, Wilson R, et al. Toward utilization of data for program management and evaluation: quality assessment of five years of health management information system data in Rwanda. Glob Health Action. 2014;7:25829. doi: 10.3402/gha.v7.25829. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
