

Risk of Arterial Thromboembolism in Patients With Cancer
- PMID: 28818202
- PMCID: PMC5667567
- DOI: 10.1016/j.jacc.2017.06.047
Risk of Arterial Thromboembolism in Patients With Cancer
Abstract
Background: The risk of arterial thromboembolism in patients with cancer is incompletely understood.
Objectives: The authors aimed to better define this epidemiological relationship, including the effects of cancer stage.
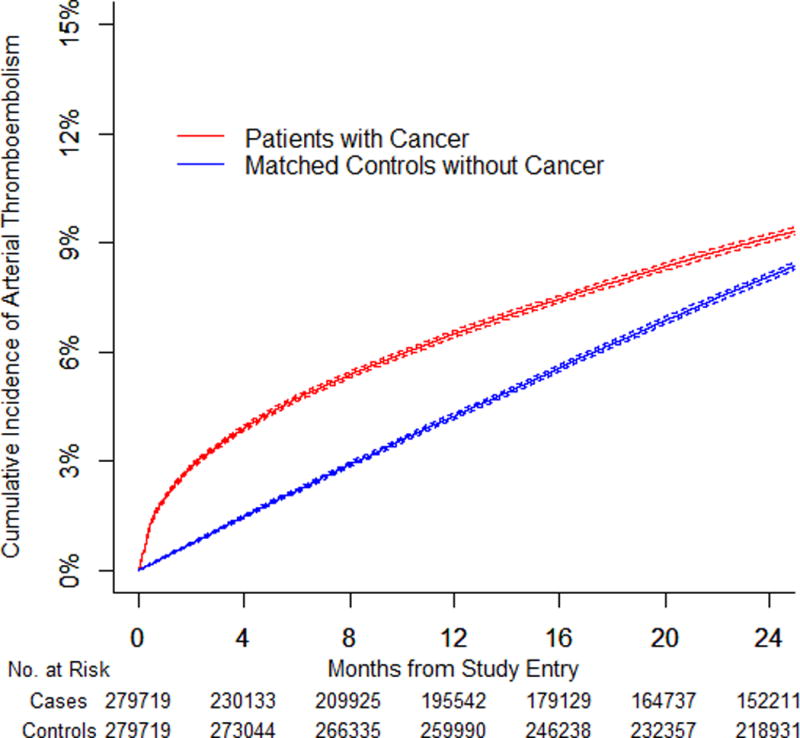
Methods: Using the Surveillance Epidemiology and End Results-Medicare linked database, the authors identified patients with a new primary diagnosis of breast, lung, prostate, colorectal, bladder, pancreatic, or gastric cancer or non-Hodgkin lymphoma from 2002 to 2011. They were individually matched by demographics and comorbidities to a Medicare enrollee without cancer, and each pair was followed through 2012. Validated diagnosis codes were used to identify arterial thromboembolism, defined as myocardial infarction or ischemic stroke. Cumulative incidence rates were calculated using competing risk survival statistics. Cox hazards analysis was used to compare rates between groups at discrete time points.
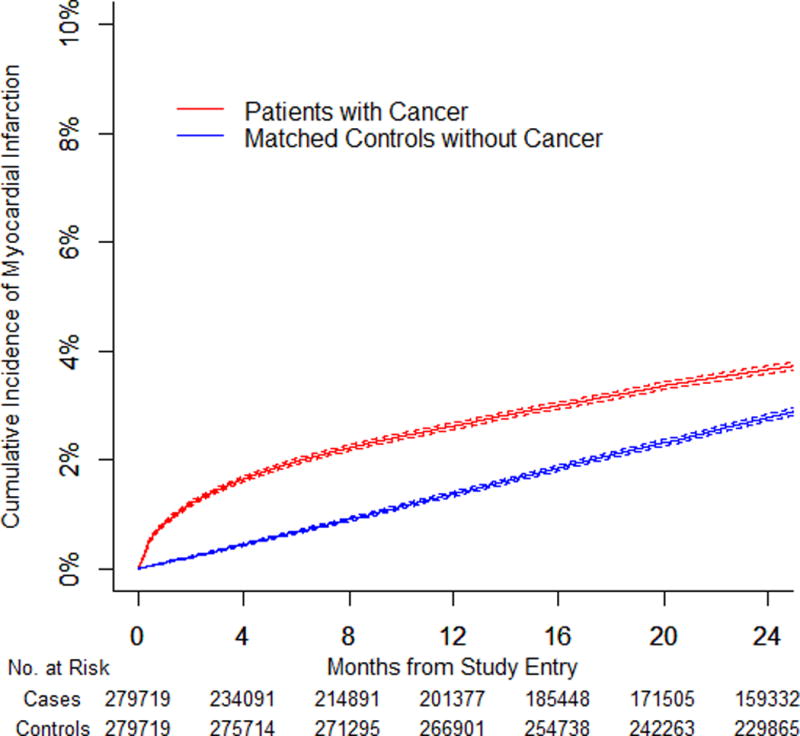
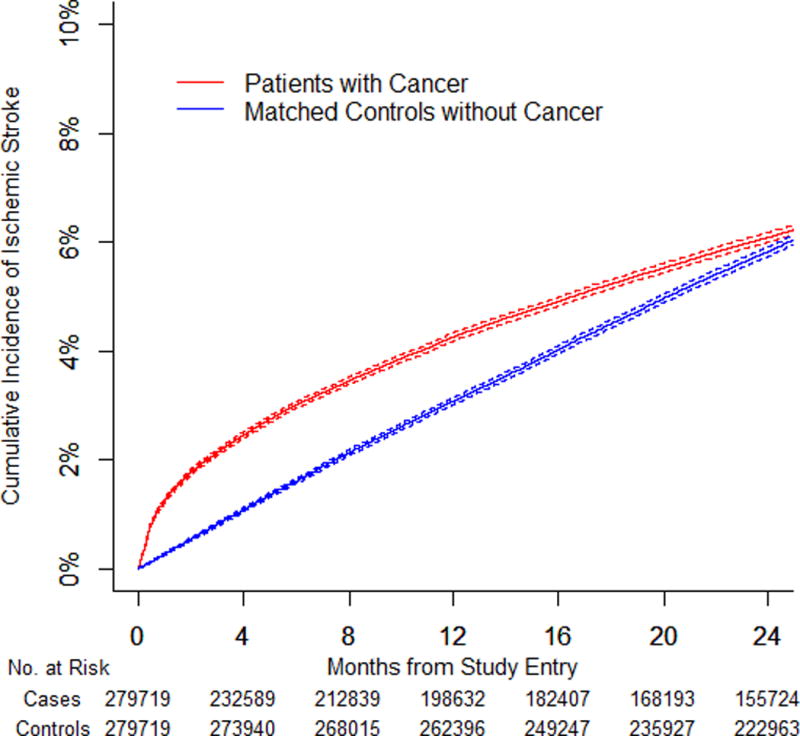
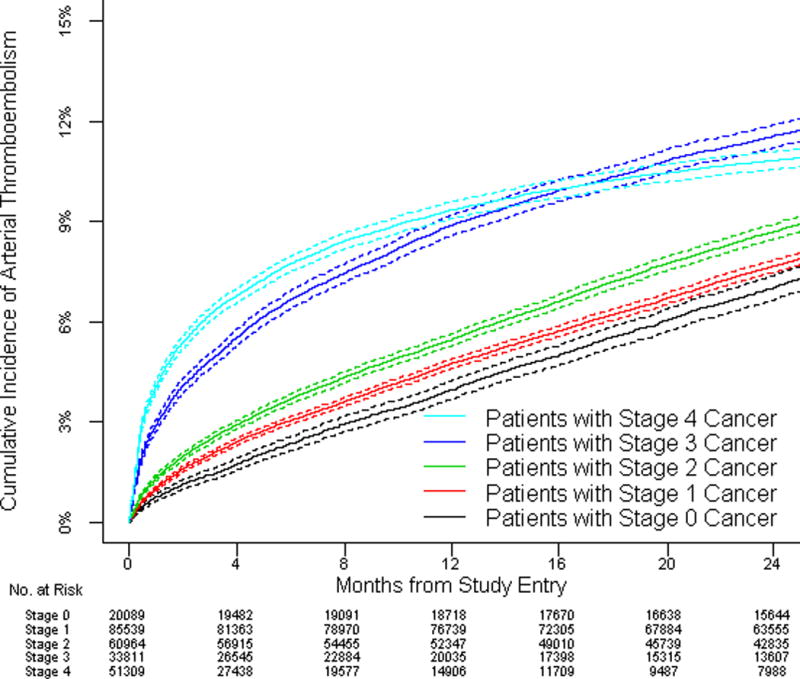
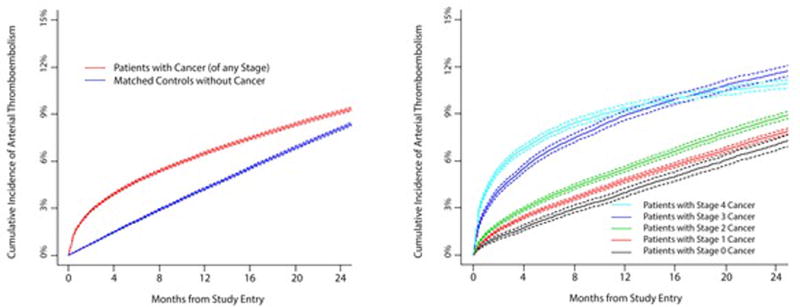
Results: The authors identified 279,719 pairs of patients with cancer and matched control patients. The 6-month cumulative incidence of arterial thromboembolism was 4.7% (95% confidence interval [CI]: 4.6% to 4.8%) in patients with cancer compared with 2.2% (95% CI: 2.1% to 2.2%) in control patients (hazard ratio [HR]: 2.2; 95% CI: 2.1 to 2.3). The 6-month cumulative incidence of myocardial infarction was 2.0% (95% CI: 1.9% to 2.0%) in patients with cancer compared with 0.7% (95% CI: 0.6% to 0.7%) in control patients (HR: 2.9; 95% CI: 2.8 to 3.1). The 6-month cumulative incidence of ischemic stroke was 3.0% (95% CI: 2.9% to 3.1%) in patients with cancer compared with 1.6% (95% CI: 1.6% to 1.7%) in control patients (HR: 1.9; 95% CI: 1.8 to 2.0). Excess risk varied by cancer type (greatest for lung), correlated with cancer stage, and generally had resolved by 1 year.
Conclusions: Patients with incident cancer face a substantially increased short-term risk of arterial thromboembolism.
Keywords: ischemic stroke; myocardial infarction; thrombosis.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cancer and Clot: Between a Rock and a Hard Place.J Am Coll Cardiol. 2017 Aug 22;70(8):939-941. doi: 10.1016/j.jacc.2017.07.719. J Am Coll Cardiol. 2017. PMID: 28818203 No abstract available.
-
Arterial Thromboembolism in Non-Hodgkin Lymphoma.J Am Coll Cardiol. 2018 Jan 16;71(2):258-259. doi: 10.1016/j.jacc.2017.09.1155. J Am Coll Cardiol. 2018. PMID: 29325650 No abstract available.
-
Recurrent Late Bioresorbable Scaffold Thrombosis as a Presenting Symptom of Underlying Cancer.J Am Coll Cardiol. 2018 Jan 16;71(2):259-260. doi: 10.1016/j.jacc.2017.10.086. J Am Coll Cardiol. 2018. PMID: 29325651 No abstract available.
-
Risk of Arterial Thrombosis in Cancer Patients: Which Role for Cancer Therapies Vascular Toxicities?J Am Coll Cardiol. 2018 Jan 16;71(2):260. doi: 10.1016/j.jacc.2017.10.087. J Am Coll Cardiol. 2018. PMID: 29325652 No abstract available.
-
Reply: Arterial Thromboembolism in Non-Hodgkin Lymphoma, as the Presentation of Occult Cancer, and With Cancer Therapies.J Am Coll Cardiol. 2018 Jan 16;71(2):260-262. doi: 10.1016/j.jacc.2017.10.088. J Am Coll Cardiol. 2018. PMID: 29325653 No abstract available.
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2013. Bethesda, MD: National Cancer Institute; 2016. Available at: http://seer.cancer.gov/csr/1975_2013/. Accessed June 23, 2017.
-
- Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA. 2005;293:715–22. - PubMed
-
- Gomes M, Khorana AA. Risk assessment for thrombosis in cancer. Semin Thromb Hemost. 2014;40:319–24. - PubMed
-
- Meschia JF, Bushnell C, Boden-Albala B, et al. American Heart Association Stroke Council. Council on Cardiovascular and Stroke Nursing. Council on Clinical Cardiology. Council on Functional Genomics and Translational Biology. Council on Hypertension Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:3754–832. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
