

Recent Advances in Targeting ROS1 in Lung Cancer
- PMID: 28818606
- PMCID: PMC5659942
- DOI: 10.1016/j.jtho.2017.08.002
Recent Advances in Targeting ROS1 in Lung Cancer
Abstract
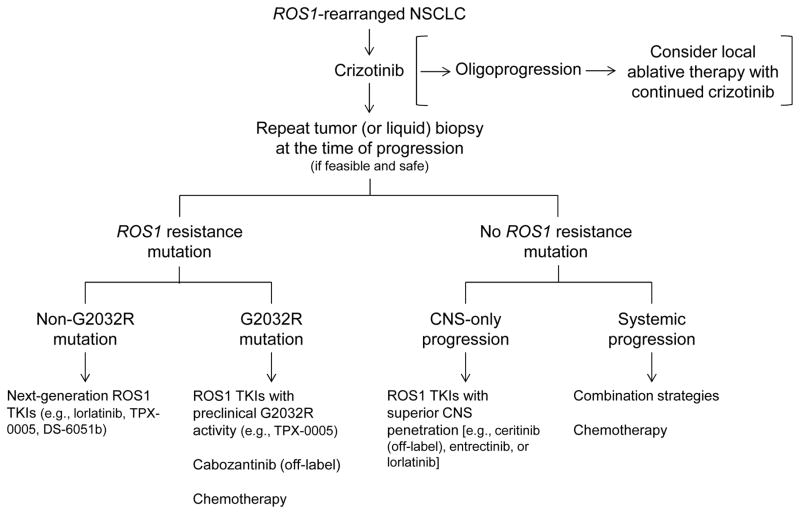
ROS1 is a validated therapeutic target in NSCLC. In a phase I study, the multitargeted MET proto-oncogene, receptor tyrosine kinase/anaplastic lymphoma kinase/ROS1 inhibitor crizotinib demonstrated remarkable efficacy in ROS1-rearranged NSCLCs and consequently gained approval by the United States Food and Drug Administration and by the European Medicines Agency in 2016. However, similar to other oncogene-driven lung cancers, ROS1-rearranged lung cancers treated with crizotinib eventually acquire resistance, leading to disease relapse. Novel ROS1 inhibitors and therapeutic strategies are therefore needed. Insights into the mechanisms of resistance to ROS1-directed tyrosine kinase inhibitors are now beginning to emerge and are helping to guide the development of new ROS1 inhibitors. This review discusses the biology and diagnosis of ROS1-rearranged NSCLC, and current and emerging treatment options for this disease. Future challenges in the field are highlighted.
Keywords: Crizotinib; Non–small cell lung cancer; ROS1 inhibitor; ROS1 rearrangement; Resistance.
Copyright © 2017 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
