

[Parathyroid carcinoma: about a case and review of the literature]
- PMID: 28819506
- PMCID: PMC5554698
- DOI: 10.11604/pamj.2017.27.85.11584
[Parathyroid carcinoma: about a case and review of the literature]
Abstract
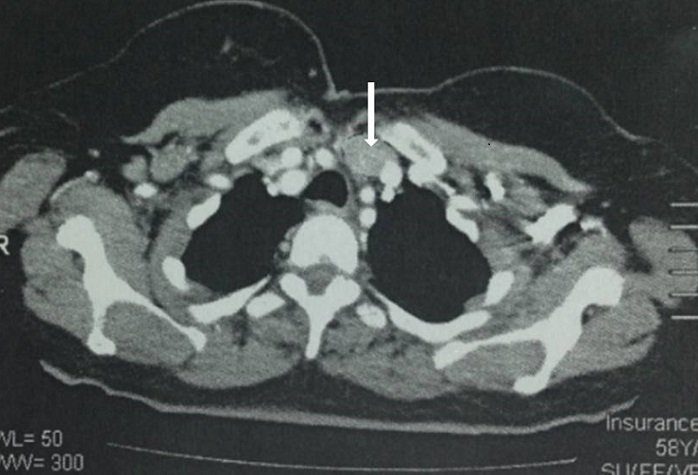
Parathyroid carcinoma is a very rare malignant tumor of the parathyroid gland. Clinically, this cancer is characterized by the presence of severe primary hyperparathyroidism. Diagnosis is based on histological examination but is not always easy. Surgery is the treatment of choice. We report the case of a 59-year old woman with a personal history of arterial hypertension and of recurrent renal lithiasis, presenting with diffuse bone pain associated with asthenia. Neck examination showed hard basi-cervical swelling with nonpalpable lower edge. Laboratory tests showed hypercalcaemia 4.1 mmol/l, hyperparathyroidism with very high parathyroid hormone (PTH) value (1088 pg/ml or 13 times normal). Technetium-99m-sestamibi scintigraphy showed fixed MIBI abnormality in the projection of the left inferior parathyroid. The patient underwent left inferior parathyroidectomy, with ipsilateral mediastinal-recurrent nerve dissection. The postoperative course was marked by normalization of plasma calcium and THP. Anatomopathological examination showed parathyroid carcinoma. The diagnosis of parathyroid carcinoma is generally based on the combination of biological, radiological and histological signs. The severity of this pathology is due to severe hypercalcaemia and to the risk of recurrence and distant metastases, justifying prolonged monitoring.
Le carcinome parathyroïdien est une tumeur maligne, très rare, de la glande parathyroïde. Cliniquement, ce cancer se présente souvent par un tableau d'hyperparathyroïdie primaire sévère. Le diagnostic est histologique mais n'est pas toujours aisé. Le traitement est basé sur la chirurgie. Femme âgée de 59 ans, aux antécédents d'hypertension artérielle, et de lithiases rénales récidivantes, consultait pour des douleurs osseuses diffuses avec asthénie. L'examen du cou a trouvé une tuméfaction basi-cervicale dure et à bord inférieur non palpable. A la biologie: hypercalcémie à 4,1 mmol/l, une hyperparathyroïdie avec valeur de parathormone (PTH) très élevée à 1088 pg/ml soit 13 fois la normale. La scintigraphie au Technétium-99m-sestamibi a montré une plage de fixation anormale de MIBI en projection de la parathyroïde inférieure gauche. Une parathyroïdectomie inférieure gauche, avec évidement médiastino-récurrentiel homolatéral ont été réalisés. Les suites opératoires étaient marquées par la normalisation de la calcémie et de la PTH. L'anatomopathologie était en faveur d'un carcinome parathyroïdien. Le diagnostic de carcinome parathyroïdien est généralement établi sur la conjonction de signes radiologiques biologiques et histologiques. La gravité de cette pathologie est due à l'hypercalcémie sévère et au risque de récidive et de métastases à distance justifiant la surveillance prolongée.
Keywords: Parathyroid; carcinoma; primary hyperparathyroidism.
Figures

References
-
- Betea D, Potorac I, Beckers A. Parathyroid carcinoma: Challenges in diagnosis and treatment. Ann Endocrinol (Paris). 2015;76(2):169–177. - PubMed
-
- Jakoubkova S, Vokurka J, Cap J, Ryska A. Parathyroid carcinoma: clinical presentation and treatment. International Congress Series. 1240. 2003:991–995.
-
- Kassahun WT, Jonas S. Focus on parathyroid carcinoma. Int J Surg. 2011;9:13–19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
