

The Impact of Introducing Malaria Rapid Diagnostic Tests on Fever Case Management: A Synthesis of Ten Studies from the ACT Consortium
- PMID: 28820705
- PMCID: PMC5637593
- DOI: 10.4269/ajtmh.16-0955
The Impact of Introducing Malaria Rapid Diagnostic Tests on Fever Case Management: A Synthesis of Ten Studies from the ACT Consortium
Abstract
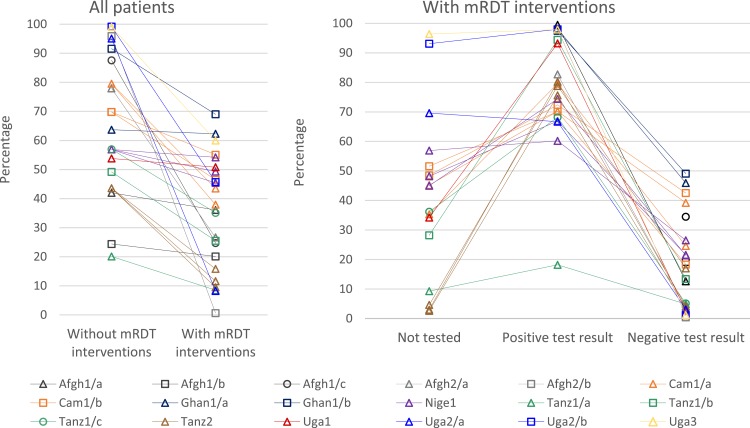
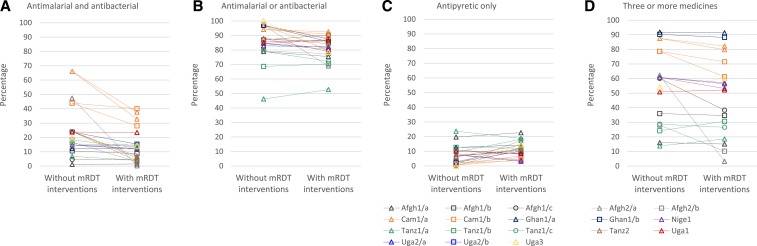
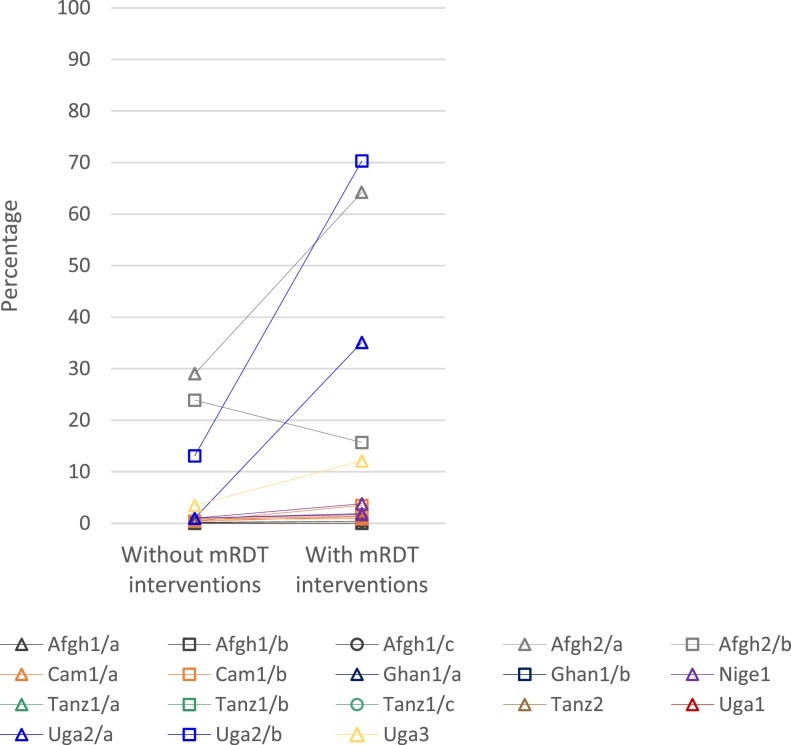
Since 2010, the World Health Organization has been recommending that all suspected cases of malaria be confirmed with parasite-based diagnosis before treatment. These guidelines represent a paradigm shift away from presumptive antimalarial treatment of fever. Malaria rapid diagnostic tests (mRDTs) are central to implementing this policy, intended to target artemisinin-based combination therapies (ACT) to patients with confirmed malaria and to improve management of patients with nonmalarial fevers. The ACT Consortium conducted ten linked studies, eight in sub-Saharan Africa and two in Afghanistan, to evaluate the impact of mRDT introduction on case management across settings that vary in malaria endemicity and healthcare provider type. This synthesis includes 562,368 outpatient encounters (study size range 2,400-432,513). mRDTs were associated with significantly lower ACT prescription (range 8-69% versus 20-100%). Prescribing did not always adhere to malaria test results; in several settings, ACTs were prescribed to more than 30% of test-negative patients or to fewer than 80% of test-positive patients. Either an antimalarial or an antibiotic was prescribed for more than 75% of patients across most settings; lower antimalarial prescription for malaria test-negative patients was partly offset by higher antibiotic prescription. Symptomatic management with antipyretics alone was prescribed for fewer than 25% of patients across all scenarios. In community health worker and private retailer settings, mRDTs increased referral of patients to other providers. This synthesis provides an overview of shifts in case management that may be expected with mRDT introduction and highlights areas of focus to improve design and implementation of future case management programs.
Figures


References
-
- World Health Organization , 2011. Universal Access to Malaria Diagnostic Testing: An Operational Manual. Geneva, Switzerland: World Health Organization.
-
- World Health Organization , 2010. Guidelines for the Treatment of Malaria. 2nd edition. Geneva, Switzerland: World Health Organization.
-
- Mabey D, Peeling RW, Ustianowski A, Perkins MD, 2004. Diagnostics for the developing world. Nat Rev Microbiol 2: 231–240. - PubMed
-
- UNITAID , 2016. Malaria Diagnostics Landscape Update. Geneva, Switzerland: World Health Organization for the UNITAID Secretariat.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
