

Decompressive craniectomy in the management of intracranial hypertension after traumatic brain injury: a systematic review and meta-analysis
- PMID: 28821777
- PMCID: PMC5562822
- DOI: 10.1038/s41598-017-08959-y
Decompressive craniectomy in the management of intracranial hypertension after traumatic brain injury: a systematic review and meta-analysis
Abstract
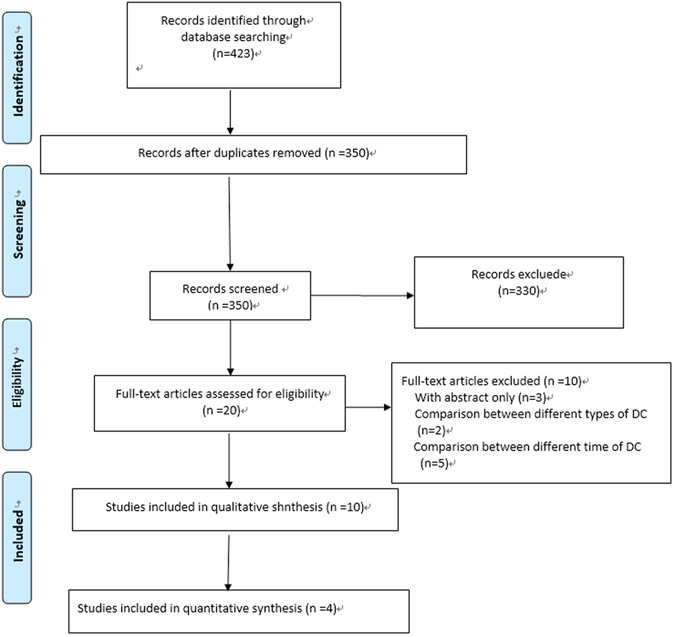
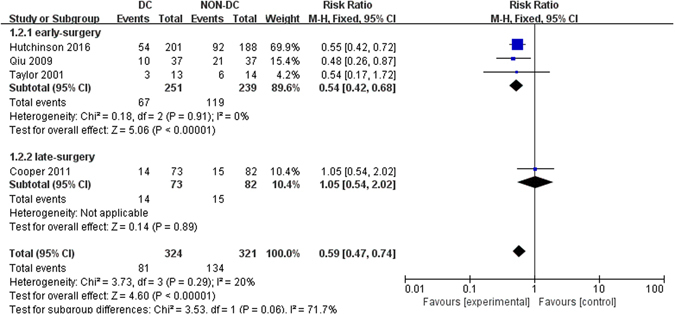
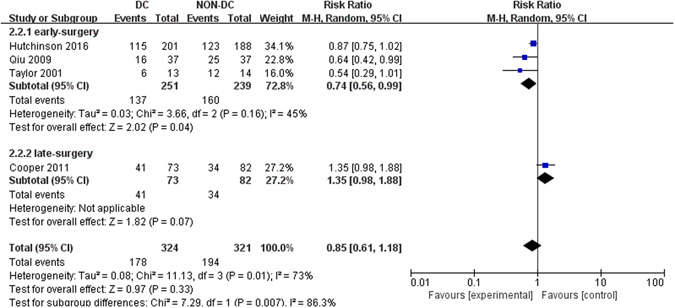
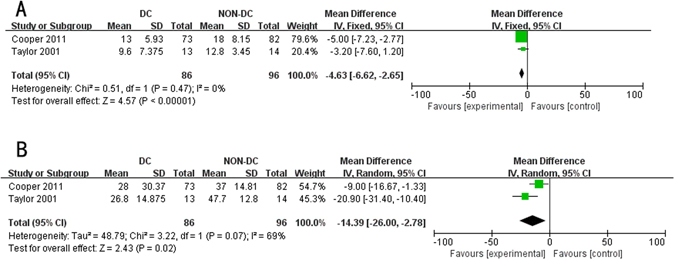
We aim to perform a systematic review and meta-analysis to examine the prognostic value of decompressive craniectomy (DC) in patients with traumatic intracranial hypertension. PubMed, EMBASE, Cochrane Controlled Trials Register, Web of Science, http://clinicaltrials.gov/ were searched for eligible studies. Ten studies were included in the systematic review, with four randomized controlled trials involved in the meta-analysis, where compared with medical therapies, DC could significantly reduce mortality rate [risk ratio (RR), 0.59; 95% confidence interval (CI), 0.47-0.74, P < 0.001], lower intracranial pressure (ICP) [mean difference (MD), -2.12 mmHg; 95% CI, -2.81 to -1.43, P < 0.001], decrease the length of ICU stay (MD, -4.63 days; 95% CI, -6.62 to -2.65, P < 0.001) and hospital stay (MD, -14.39 days; 95% CI, -26.00 to -2.78, P = 0.02), but increase complications rate (RR, 1.94; 95% CI, 1.31-2.87, P < 0.001). No significant difference was detected for Glasgow Outcome Scale at six months (RR, 0.85; 95% CI, 0.61-1.18, P = 0.33), while in subgroup analysis, early DC would possibly result in improved prognosis (P = 0.04). Results from observational studies supported pooled results except prolonged length of ICU and hospital stay. Conclusively, DC seemed to effectively lower ICP, reduce mortality rate but increase complications rate, while its benefit on functional outcomes was not statistically significant.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Hutchinson PJ, et al. Intracranial pressure monitoring in severe traumatic brain injury. BMJ (Clinical research ed.) 2013;346 - PubMed
-
- Sahuquillo J, Arikan F. Decompressive craniectomy for the treatment of refractory high intracranial pressure in traumatic brain injury. The Cochrane database of systematic reviews, Cd003983. 2006 - PubMed
-
- Bratton SL, et al. Guidelines for the management of severe traumatic brain injury. XV. Steroids. Journal of neurotrauma. 2007;24(Suppl 1):S91–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
