

Visceral adiposity index is strongly associated with hyperuricemia independently of metabolic health and obesity phenotypes
- PMID: 28821853
- PMCID: PMC5562916
- DOI: 10.1038/s41598-017-09455-z
Visceral adiposity index is strongly associated with hyperuricemia independently of metabolic health and obesity phenotypes
Abstract
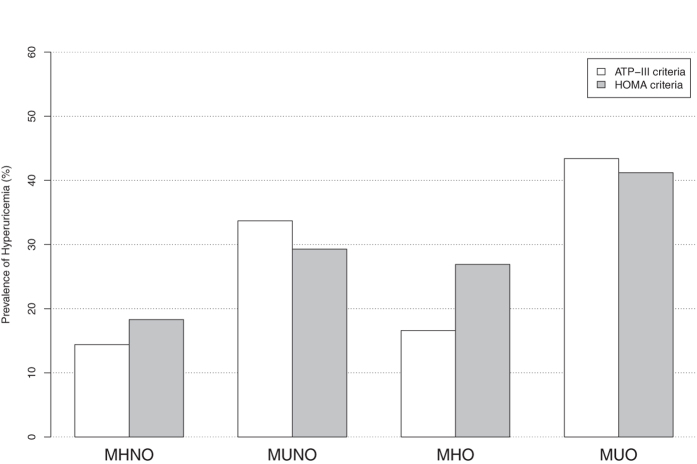
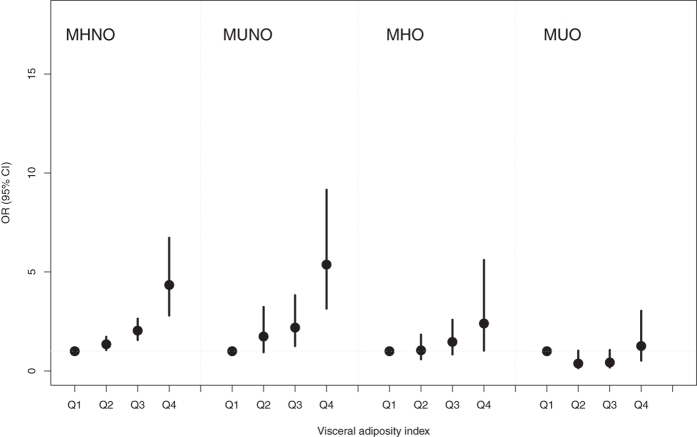
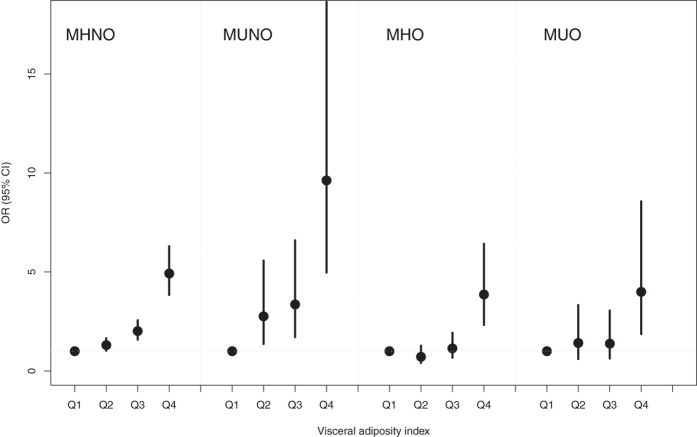
Visceral adiposity index (VAI) is a novel sex-specific index for visceral adipose function; however the association between VAI and hyperuricemia in China is unknown. We aimed to investigate this association, also whether it was independent of metabolic health and obesity phenotypes. 7632 adult subjects from the China Health and Nutrition Survey 2009 were retained. Subjects were categorized into four obesity phenotypes based on a cross-classification of BMI and metabolic health status by two representative criteria. VAI was the best predictors for hyperuricemia irrespective of obesity phenotypes, with area under curve (AUC) ranging 0.665-0.719. The odd ratio (OR) for hyperuricemia in the highest quartile of the VAI were 6.93 (95% CI 5.79-8.29) after adjusting for age and gender. Following further adjustments for metabolic obesity phenotypes and lifestyle confounders, the ORs were 4.88 (3.92-6.09) and 5.65 (4.68-6.82) according to these two criteria, respectively. A similar significant pattern was still found even after adjustment for blood pressure and other cardiovascular risks. Within each metabolic obesity phenotype, the significant association between VAI and hyperuricemia was consistently evident. In conclusion, the association of the VAI with hyperuricemia was significant, especially this association was independent of metabolic health and obesity phenotypes in the Chinese population.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Positively increased visceral adiposity index in hyperuricemia free of metabolic syndrome.Lipids Health Dis. 2018 May 7;17(1):101. doi: 10.1186/s12944-018-0761-1. Lipids Health Dis. 2018. PMID: 29734946 Free PMC article.
-
Lipid accumulation product and visceral adiposity index are effective markers for identifying the metabolically obese normal-weight phenotype.Acta Diabetol. 2015 Oct;52(5):855-63. doi: 10.1007/s00592-015-0715-2. Epub 2015 Feb 19. Acta Diabetol. 2015. PMID: 25690647
-
Visceral adiposity index predicts the conversion of metabolically healthy obesity to an unhealthy phenotype.PLoS One. 2017 Jun 23;12(6):e0179635. doi: 10.1371/journal.pone.0179635. eCollection 2017. PLoS One. 2017. PMID: 28644850 Free PMC article.
-
Visceral adiposity index as a predictor for type 2 diabetes mellitus in Asian population: A systematic review.Diabetes Metab Syndr. 2019 Mar-Apr;13(2):1231-1235. doi: 10.1016/j.dsx.2019.01.056. Epub 2019 Jan 30. Diabetes Metab Syndr. 2019. PMID: 31336469
-
Converging Relationships of Obesity and Hyperuricemia with Special Reference to Metabolic Disorders and Plausible Therapeutic Implications.Diabetes Metab Syndr Obes. 2020 Mar 30;13:943-962. doi: 10.2147/DMSO.S232377. eCollection 2020. Diabetes Metab Syndr Obes. 2020. PMID: 32280253 Free PMC article. Review.
Cited by
-
Changes in Adipose Tissue Distribution and Association between Uric Acid and Bone Health during Menopause Transition.Int J Mol Sci. 2019 Dec 14;20(24):6321. doi: 10.3390/ijms20246321. Int J Mol Sci. 2019. PMID: 31847375 Free PMC article.
-
Association between hyperuricemia and nontraditional adiposity indices.Clin Rheumatol. 2019 Apr;38(4):1055-1062. doi: 10.1007/s10067-018-4374-x. Epub 2018 Nov 29. Clin Rheumatol. 2019. PMID: 30498873
-
Association between new anthropometric parameters and arterial stiffness based on brachial-ankle pulse wave velocity.Diabetes Metab Syndr Obes. 2019 Sep 3;12:1727-1733. doi: 10.2147/DMSO.S211542. eCollection 2019. Diabetes Metab Syndr Obes. 2019. PMID: 31564940 Free PMC article.
-
Triglyceride Glucose Index Is More Closely Related to Hyperuricemia Than Obesity Indices in the Medical Checkup Population in Xinjiang, China.Front Endocrinol (Lausanne). 2022 Mar 2;13:861760. doi: 10.3389/fendo.2022.861760. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35311243 Free PMC article.
-
Association between magnesium depletion score and prevalence of hyperuricemia in American adults: a study based on NHANES 2007-2018.Front Endocrinol (Lausanne). 2025 Feb 6;16:1438639. doi: 10.3389/fendo.2025.1438639. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 39980850 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
