

Not All Orbitopathy Is Graves': Discussion of Cases and Review of Literature
- PMID: 28824545
- PMCID: PMC5534452
- DOI: 10.3389/fendo.2017.00184
Not All Orbitopathy Is Graves': Discussion of Cases and Review of Literature
Abstract
Introduction: Graves' orbitopathy is the extra thyroidal manifestation of Graves' disease and the most common cause of exophthalmos. It is also known as thyroid-associated orbitopathy (TAO) as it occasionally occurs in euthyroid or hypothyroid patients with chronic thyroiditis. 5% of patients with Graves' orbitopathy can be euthyroid or hypothyroid as they have low titers of anti-thyrotropin-receptor antibodies, which are difficult to detect in some assays. Orbitopathy has also been seen in a small percentage of patients with Hashimotos thyroiditis. The eye involvement in Graves' is frequently bilateral and symmetric. These patients pose few diagnostic difficulties when the ocular findings occur concomitantly with the thyroid disease. However, when unilateral and asymmetric ocular findings occur with normal or mildly abnormal thyroid function tests, alternate etiologies should also be pursued. We aim to discuss some conditions like sarcoidosis, lymphoma, orbital pseudotumor, and orbital malignancy that mimic TAO.
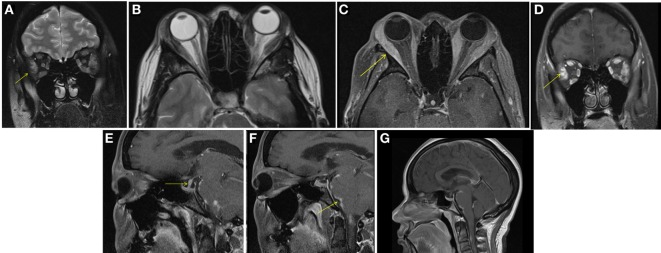
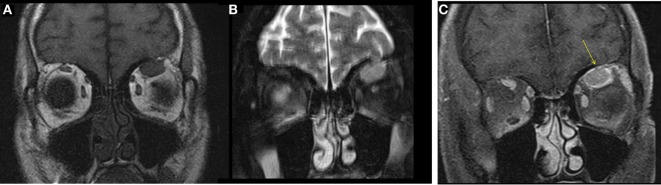
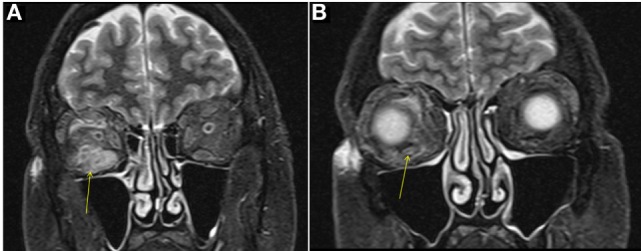
Cases: Three patients were referred to us with concern for Graves' orbitopathy. After further work-up, we diagnosed the first patient with specific orbital myositis from sarcoidosis. Our second patient had CD10-positive B-cell lymphoma. Our third patient had orbitopathy likely secondary to Hashimotos or orbital pseudotumor.
Conclusion: Our cases and discussion describe some other conditions that clinically mimic TAO and the importance of pursuing further work-up for accurate diagnosis when presentation of orbitopathy is atypical.
Keywords: Graves’ orbitopathy; differential of thyroid-associated orbitopathy; orbital lymphoma; orbitopathy; sarcoid orbitopathy.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources