

Image-Guided Transurethral Resection of Bladder Tumors - Current Practice and Future Outlooks
- PMID: 28824942
- PMCID: PMC5545914
- DOI: 10.3233/BLC-170119
Image-Guided Transurethral Resection of Bladder Tumors - Current Practice and Future Outlooks
Abstract
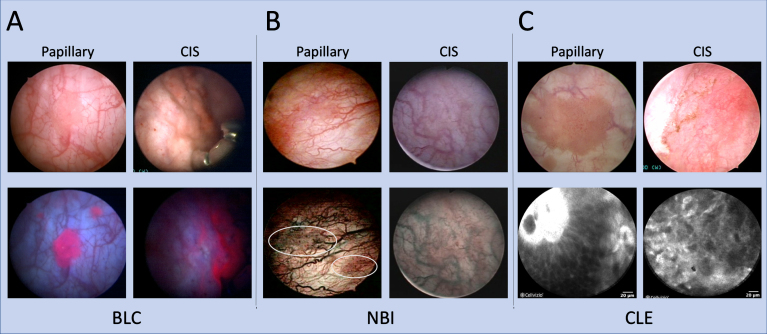
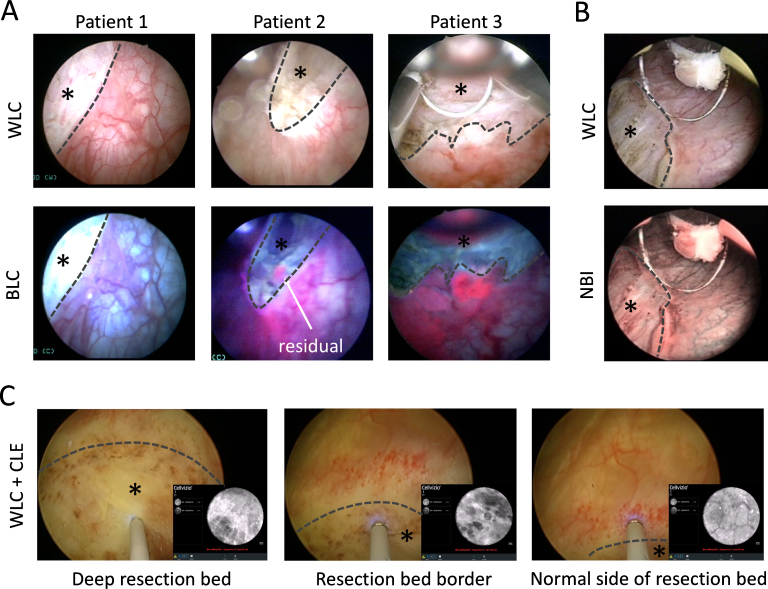
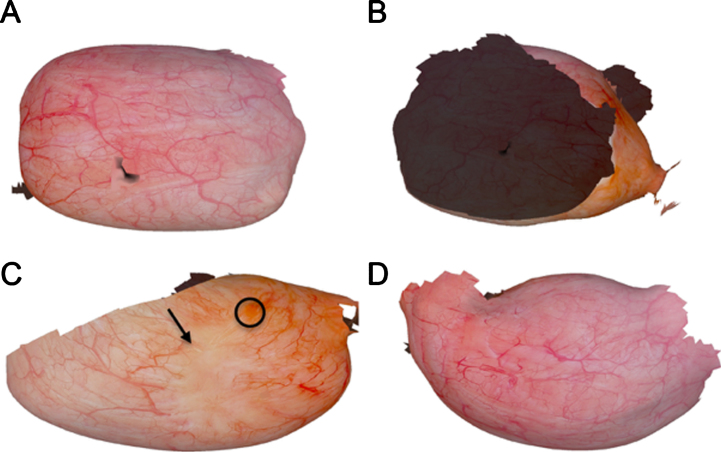
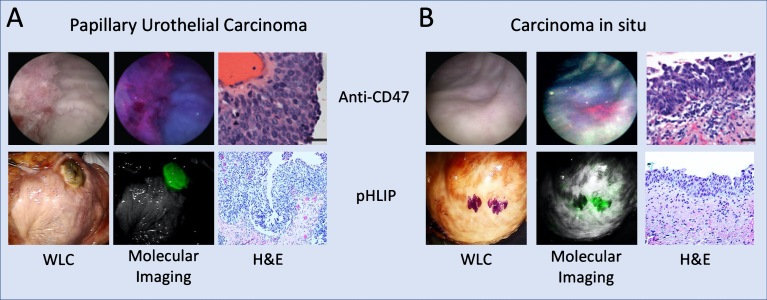
Transurethral resection of bladder tumor (TURBT) under white light cystoscopy (WLC) is the cornerstone for the diagnosis, removal and local staging of non-muscle invasive bladder cancer (NMIBC). Despite technological improvements over the decades, significant shortcomings remain with WLC for tumor detection, thereby impacting the surgical quality and contributing to tumor recurrence and progression. Enhanced cystoscopy modalities such as blue light cystoscopy (BLC) and narrow band imaging (NBI) aid resections by highlighting tumors that might be missed on WLC. Optical biopsy technologies such as confocal laser endomicroscopy (CLE) and optical coherence tomography (OCT) characterize tissue in real-time to ensure a more thorough resection. New resection techniques, particularly en bloc resection, are actively under investigation to improve the overall quality of resections and aid pathologic interpretation. Moreover, new image processing computer algorithms may improve perioperative planning and longitudinal follow-up. Clinical translation of molecular imaging agents is also on the horizon to improve optical diagnosis of bladder cancer. This review focuses on emerging technologies that can impact the quality of TURBT to improve the overall management of NMIBC.
Keywords: Urinary bladder neoplasms; antigens CD47; computer-assisted; confocal microscopy; cystoscopy; hexaminolevulinic acid; laser surgery; molecular imaging; narrow band imaging; optical coherence tomography.
Figures
References
-
- Beer E. Landmark article May 28, Removal of neoplasms of the urinary bladder. By Edwin Beer. Jama 1983;250(10):1324–5. - PubMed
-
- Babjuk M, Bohle A, Burger M, Capoun O, Cohen D, Comperat EM, et al. EAU Guidelines on non-muscle-invasive urothelial carcinoma of the bladder: Update 2016. European urology 2017;71(3):447–61. - PubMed
-
- Zainfeld D, Daneshmand S. Transurethral resection of bladder tumors: Improving quality through new techniques and technologies. Current Urology Reports 2017;18(5):34. - PubMed
-
- Witjes JA. Bladder carcinoma in situ in State of the art. European Urology 2004;45(2):142–6. - PubMed
-
- Schwaibold HE, Sivalingam S, May F, Hartung R. The value of a second transurethral resection for T1 bladder cancer. BJU International 2006;97(6):1199–201. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
