

Primary Spinal Intradural Mesenchymal Chondrosarcoma with Several Local Regrowths Treated with Osteoplastic Laminotomies: A Case Report
- PMID: 28825035
- PMCID: PMC5553510
- DOI: 10.1055/s-0037-1604159
Primary Spinal Intradural Mesenchymal Chondrosarcoma with Several Local Regrowths Treated with Osteoplastic Laminotomies: A Case Report
Abstract
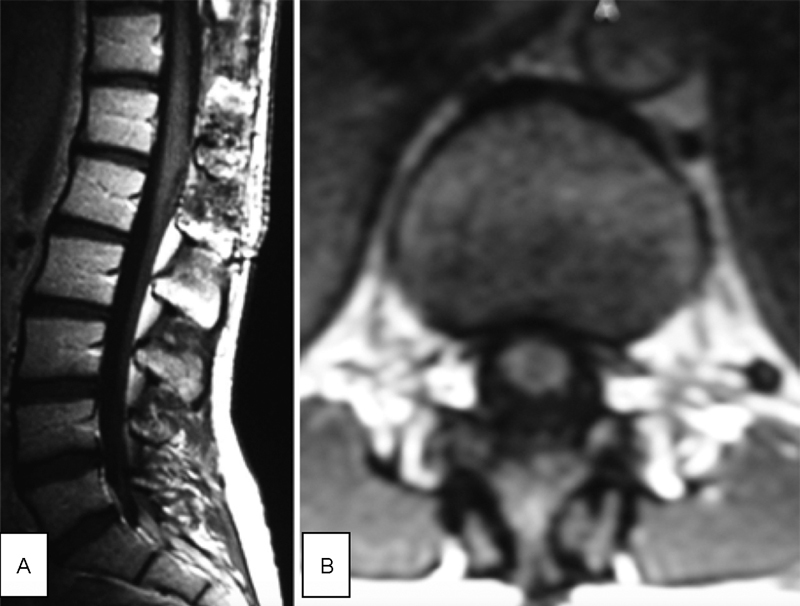
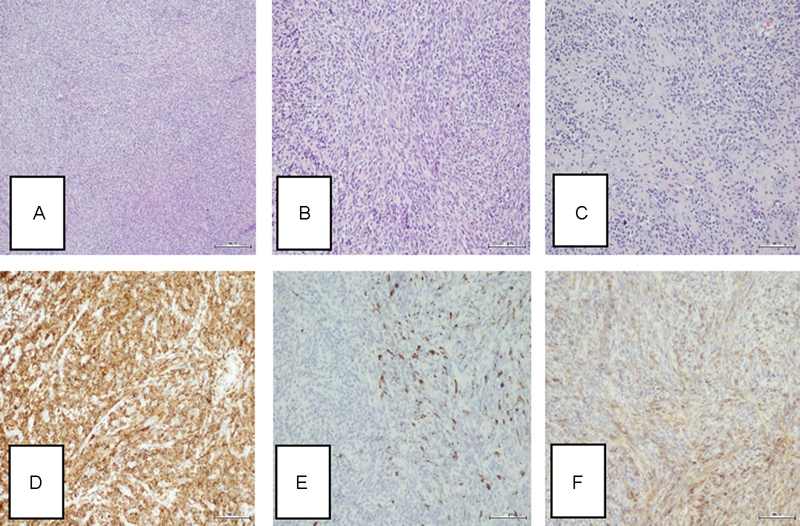
Mesenchymal chondrosarcomas (MCSs) are rare malignant tumors of the bone and soft tissues. Only a few cases of such tumors originating from the spinal canal meninges have been described in the literature. The authors report on a case of a 22-year-old woman with MCS of the arachnoid at the T12-L1 level with a 14-year-long observation. The tumor was totally resected using osteoplastic laminotomy with reconstruction of laminar roof. This small spindle cell tumor was initially microscopically suspected of synovial sarcoma, but correctly verified with widened immunophenotyping and molecular studies as MCS. At its first recurrence, the neoplasm showed microscopically a typical bimorphic pattern of small round cell component with foci of hyaline cartilage. The patient experienced three local recurrences: 4, 6, and 10 years after the initial resection, respectively. The techniques of laminotomy and relaminotomy were also used during three following operations. The repeated surgical removal, radiotherapy, and chemotherapy were the methods of complex oncological treatment. The patient remains now in complete remission, fully self-dependent with slight motor disturbance, and mild sensory deficits. Current views on the clinicopathological characteristics and treatment modalities of the chondrosarcomas of the spinal canal are discussed.
Keywords: adjuvant treatment; intradural tumor; mesenchymal chondrosarcoma; neurosurgery; spinal tumor.
Conflict of interest statement
Figures




References
-
- Guccion J G, Font R L, Enzinger F M, Zimmerman L E. Extraskeletal mesenchymal chondrosarcoma. Arch Pathol. 1973;95(05):336–340. - PubMed
-
- Lightenstein L, Bernstein D. Unusual benign and malignant chondroid tumors of bone. A survey of some mesenchymal cartilage tumors and malignant chondroblastic tumors, including a few multicentric ones, as well as many atypical benign chondroblastomas and chondromyxoid fibromas. Cancer. 1959;12:1142–1157. - PubMed
-
- Huvos A G, Rosen G, Dabska M, Marcove R C. Mesenchymal chondrosarcoma. A clinicopathologic analysis of 35 patients with emphasis on treatment. Cancer. 1983;51(07):1230–1237. - PubMed
-
- Nakashima Y, Unni K K, Shives T C, Swee R G, Dahlin D C. Mesenchymal chondrosarcoma of bone and soft tissue. A review of 111 cases. Cancer. 1986;57(12):2444–2453. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources