

Relative Incidence of Seizures and Myoclonus in Alzheimer's Disease, Dementia with Lewy Bodies, and Frontotemporal Dementia
- PMID: 28826176
- PMCID: PMC5608587
- DOI: 10.3233/JAD-170031
Relative Incidence of Seizures and Myoclonus in Alzheimer's Disease, Dementia with Lewy Bodies, and Frontotemporal Dementia
Abstract
Background: Patients with Alzheimer's disease (AD) are more prone to seizures and myoclonus, but relative risk of these symptoms among other dementia types is unknown.
Objective: To determine incidence of seizures and myoclonus in the three most common neurodegenerative dementias: AD, dementia with Lewy bodies (DLB), and frontotemporal dementia (FTD).
Methods: Our institution's medical records were reviewed for new-onset unprovoked seizures and myoclonus in patients meeting criteria for AD (n = 1,320), DLB (n = 178), and FTD (n = 348). Cumulative probabilities of developing seizures and myoclonus were compared between diagnostic groups, whereas age-stratified incidence rates were determined relative to control populations.
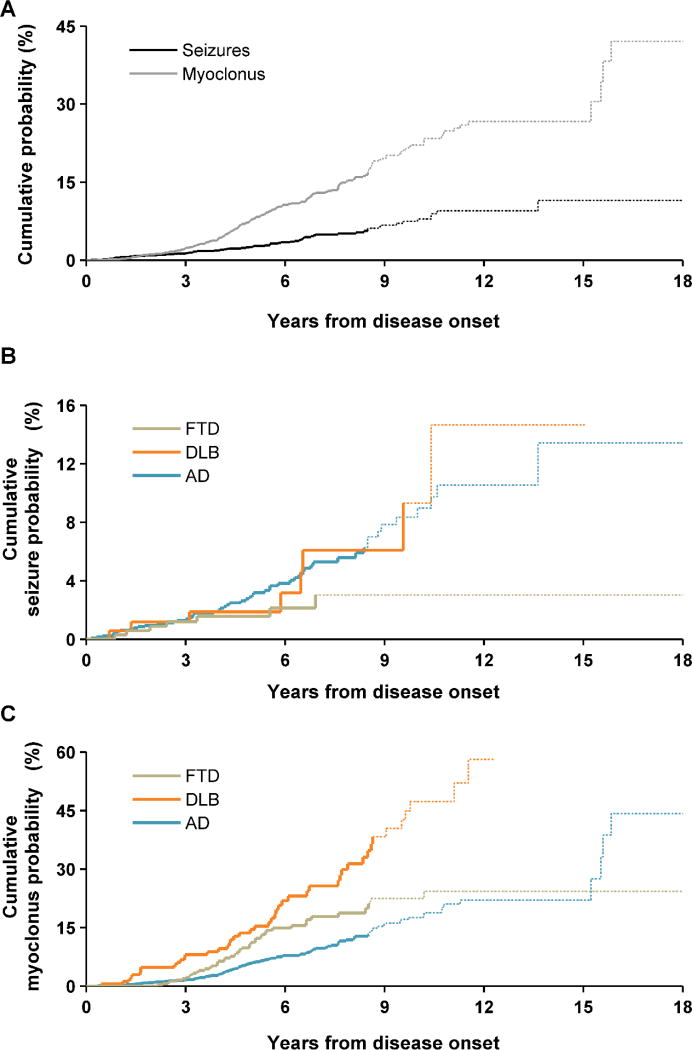
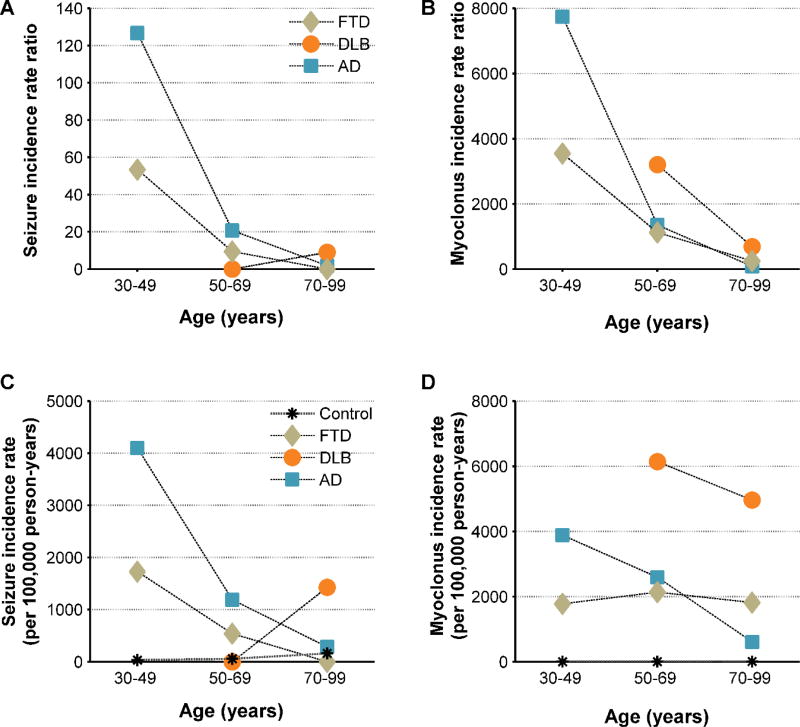
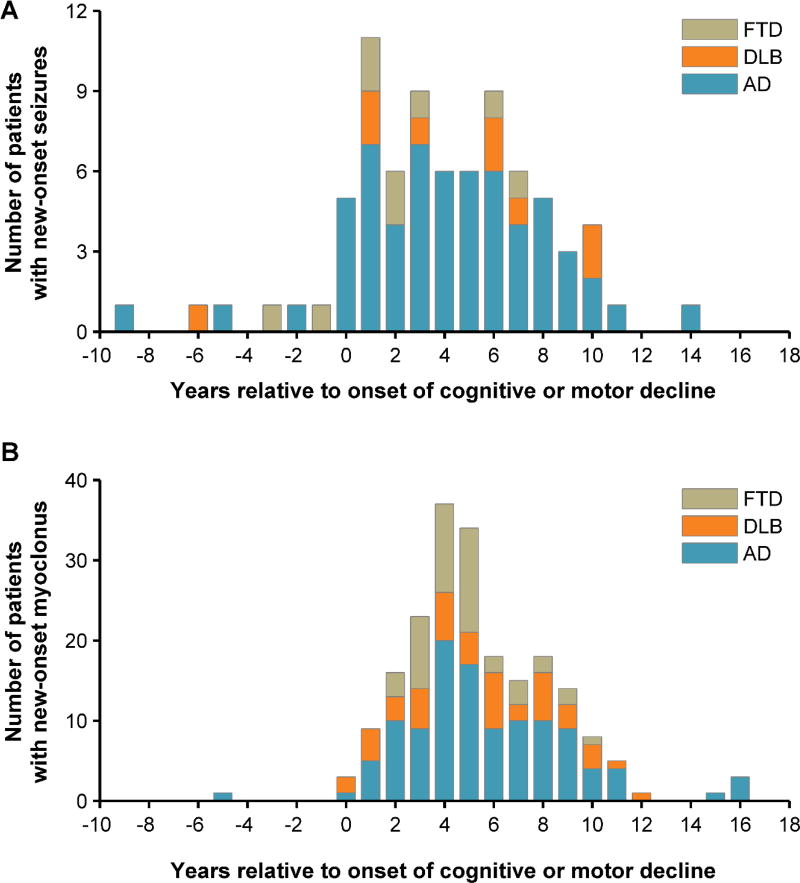
Results: The cumulative probability of developing seizures after disease onset was 11.5% overall, highest in AD (13.4%) and DLB (14.7%) and lowest in FTD (3.0%). The cumulative probability of developing myoclonus was 42.1% overall, highest in DLB (58.1%). The seizure incidence rates, relative to control populations, were nearly 10-fold in AD and DLB, and 6-fold in FTD. Relative seizure rates increased with earlier age-at-onset in AD (age <50, 127-fold; 50-69, 21-fold; 70+, 2-fold) and FTD (age <50, 53-fold; 50-69, 9-fold), and relative myoclonus rates increased with earlier age-at-onset in all groups. Seizures began an average of 3.9 years after the onset of cognitive or motor decline, and myoclonus began 5.4 years after onset.
Conclusions: Seizures and myoclonus occur with greater incidence in patients with AD, DLB, and FTD than in the general population, but rates vary with diagnosis, suggesting varied pathomechanisms of network hyperexcitability. Patients often experience these symptoms early in disease, suggesting hyperexcitability could be an important target for interventions.
Keywords: Alzheimer’s disease; dementia with Lewy bodies; epilepsy; frontotemporal dementia.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures
References
-
- Amatniek JC, Hauser WA, DelCastillo-Castaneda C, Jacobs DM, Marder K, Bell K, Albert M, Brandt J, Stern Y. Incidence and predictors of seizures in patients with Alzheimer’s disease. Epilepsia. 2006;47:867–872. - PubMed
-
- Romanelli MF, Morris JC, Ashkin K, Coben LA. Advanced Alzheimer’s disease is a risk factor for late-onset seizures. Arch Neurol. 1990;47:847–850. - PubMed
-
- Vossel KA, Beagle AJ, Rabinovici GD, Shu H, Lee SE, Naasan G, Hegde M, Cornes SB, Henry ML, Nelson AB, Seeley WW, Geschwind MD, Gorno-Tempini ML, Shih T, Kirsch HE, Garcia PA, Miller BL, Mucke L. Seizures and epileptiform activity in the early stages of Alzheimer disease. JAMA Neurol. 2013;70:1158–1166. - PMC - PubMed
-
- Cretin B, Sellal F, Philippi N, Bousiges O, Di Bitonto L, Martin-Hunyadi C, Blanc F. Epileptic Prodromal Alzheimer’s Disease, a Retrospective Study of 13 New Cases: Expanding the Spectrum of Alzheimer’s Disease to an Epileptic Variant. J Alzheimers Dis 2016 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
