

A score to predict and stratify risk of tuberculosis in adult contacts of tuberculosis index cases: a prospective derivation and external validation cohort study
- PMID: 28827142
- PMCID: PMC7611139
- DOI: 10.1016/S1473-3099(17)30447-4
A score to predict and stratify risk of tuberculosis in adult contacts of tuberculosis index cases: a prospective derivation and external validation cohort study
Erratum in
-
Corrections.Lancet Infect Dis. 2017 Nov;17(11):1117. doi: 10.1016/S1473-3099(17)30573-X. Epub 2017 Sep 13. Lancet Infect Dis. 2017. PMID: 28918082 No abstract available.
Abstract
Background: Contacts of tuberculosis index cases are at increased risk of developing tuberculosis. Screening, preventive therapy, and surveillance for tuberculosis are underused interventions in contacts, particularly adults. We developed a score to predict risk of tuberculosis in adult contacts of tuberculosis index cases.
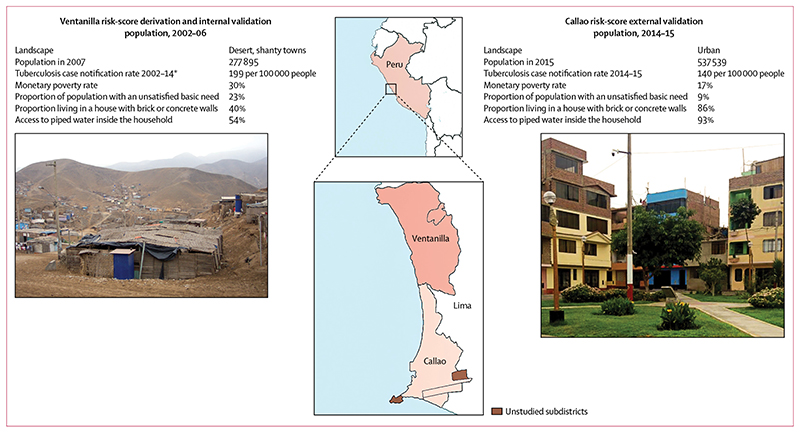
Methods: In 2002-06, we recruited contacts aged 15 years or older of index cases with pulmonary tuberculosis who lived in desert shanty towns in Ventanilla, Peru. We followed up contacts for tuberculosis until February, 2016. We used a Cox proportional hazards model to identify index case, contact, and household risk factors for tuberculosis from which to derive a score and classify contacts as low, medium, or high risk. We validated the score in an urban community recruited in Callao, Peru, in 2014-15.
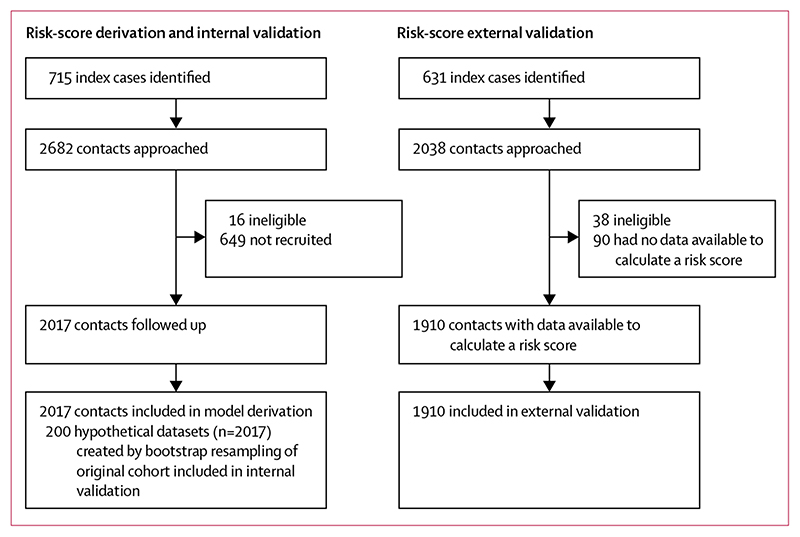
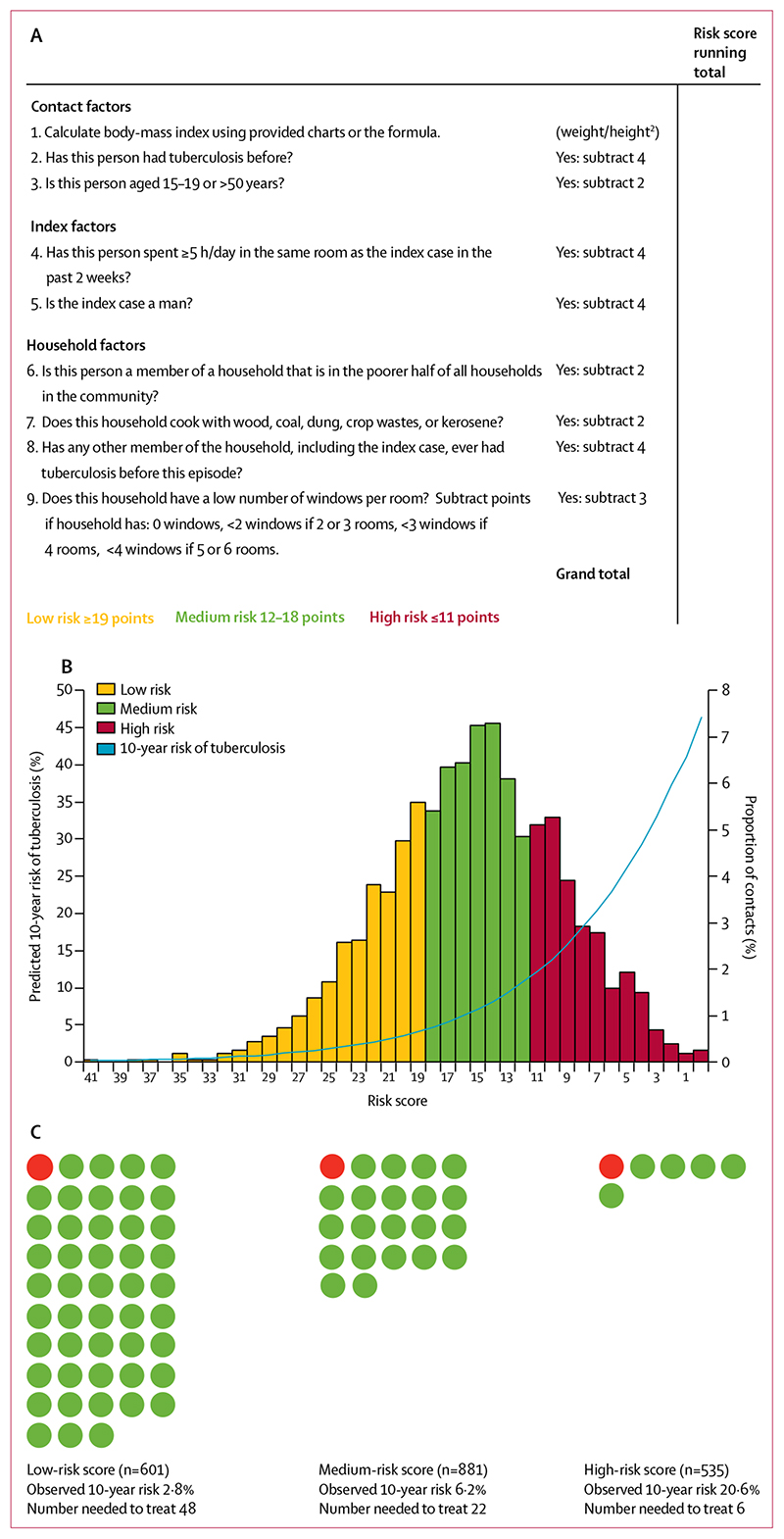
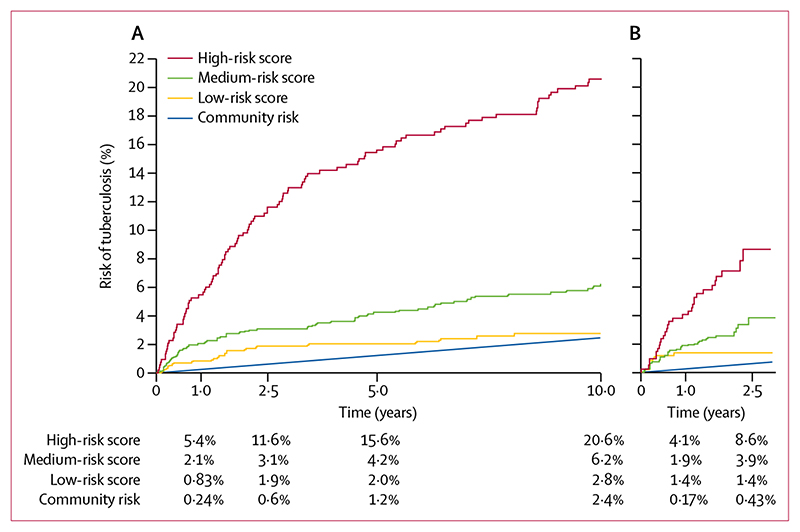
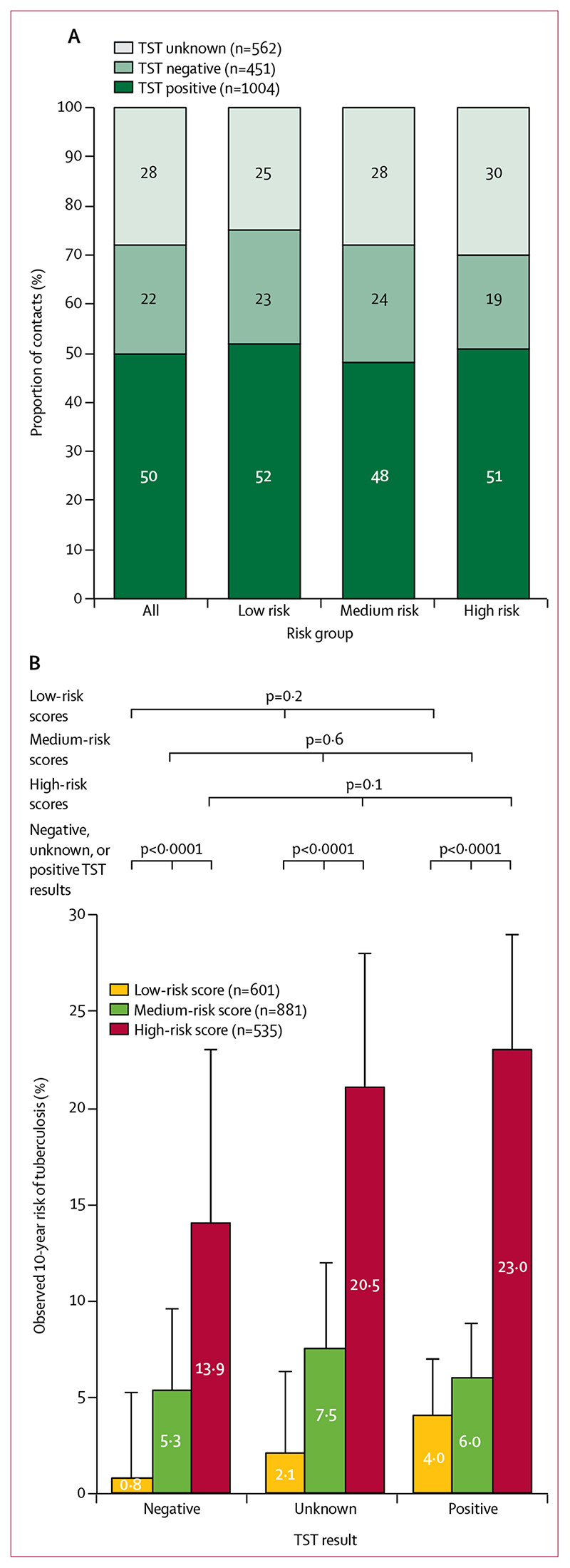
Findings: In the derivation cohort, we identified 2017 contacts of 715 index cases, and median follow-up was 10·7 years (IQR 9·5-11·8). 178 (9%) of 2017 contacts developed tuberculosis during 19 147 person-years of follow-up (incidence 0·93 per 100 person-years, 95% CI 0·80-1·08). Risk factors for tuberculosis were body-mass index, previous tuberculosis, age, sustained exposure to the index case, the index case being in a male patient, lower community household socioeconomic position, indoor air pollution, previous tuberculosis among household members, and living in a household with a low number of windows per room. The 10-year risks of tuberculosis in the low-risk, medium-risk, and high-risk groups were, respectively, 2·8% (95% CI 1·7-4·4), 6·2% (4·8-8·1), and 20·6% (17·3-24·4). The 535 (27%) contacts classified as high risk accounted for 60% of the tuberculosis identified during follow-up. The score predicted tuberculosis independently of tuberculin skin test and index-case drug sensitivity results. In the external validation cohort, 65 (3%) of 1910 contacts developed tuberculosis during 3771 person-years of follow-up (incidence 1·7 per 100 person-years, 95% CI 1·4-2·2). The 2·5-year risks of tuberculosis in the low-risk, medium-risk, and high-risk groups were, respectively, 1·4% (95% CI 0·7-2·8), 3·9% (2·5-5·9), and 8·6%· (5·9-12·6).
Interpretation: Our externally validated risk score could predict and stratify 10-year risk of developing tuberculosis in adult contacts, and could be used to prioritise tuberculosis control interventions for people most likely to benefit.
Funding: Wellcome Trust, Department for International Development Civil Society Challenge Fund, Joint Global Health Trials consortium, Bill & Melinda Gates Foundation, Imperial College National Institutes of Health Research Biomedical Research Centre, Foundation for Innovative New Diagnostics, Sir Halley Stewart Trust, WHO, TB REACH, and Innovation for Health and Development.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
Comment in
-
Tuberculosis-making predictions, especially about the future.Lancet Infect Dis. 2017 Nov;17(11):1106-1107. doi: 10.1016/S1473-3099(17)30492-9. Epub 2017 Aug 18. Lancet Infect Dis. 2017. PMID: 28827143 Free PMC article. No abstract available.
-
Prediction and prevention of tuberculosis in contacts.Lancet Infect Dis. 2017 Dec;17(12):1237-1238. doi: 10.1016/S1473-3099(17)30641-2. Lancet Infect Dis. 2017. PMID: 29173880 No abstract available.
-
Prediction and prevention of tuberculosis in contacts.Lancet Infect Dis. 2017 Dec;17(12):1237. doi: 10.1016/S1473-3099(17)30640-0. Lancet Infect Dis. 2017. PMID: 29173881 No abstract available.
-
Prediction and prevention of tuberculosis in contacts - Authors' reply.Lancet Infect Dis. 2017 Dec;17(12):1238-1239. doi: 10.1016/S1473-3099(17)30642-4. Lancet Infect Dis. 2017. PMID: 29173882 No abstract available.
-
Tuberculosis in adult contacts of an index case: Can we predict in India?Natl Med J India. 2018 Mar-Apr;31(2):99-100. doi: 10.4103/0970-258X.253169. Natl Med J India. 2018. PMID: 30829226 No abstract available.
References
-
- WHO. Recommendations for investigating contacts of persons with infectious tuberculosis in low- and middle-income countries. World Health Organization; Geneva: 2012. - PubMed
-
- Alsdurf H, Hill PC, Matteelli A, Getahun H, Menzies D. The cascade of care in diagnosis and treatment of latent tuberculosis infection: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16:1269–78. - PubMed
-
- Tebruegge M, Bogyi M, Soriano-Arandes A, Kampmann B. Shortage of purified protein derivative for tuberculosis testing. Lancet. 2014;384:2026. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
