

Assessment of healthcare delivery in the early management of bacterial meningitis in UK young infants: an observational study
- PMID: 28827241
- PMCID: PMC5724087
- DOI: 10.1136/bmjopen-2016-015700
Assessment of healthcare delivery in the early management of bacterial meningitis in UK young infants: an observational study
Abstract
Objective: To define early presenting features of bacterial meningitis in young infants in England and to review the adequacy of individual case management as compared with relevant national guidelines and an expert panel review.
Design: Retrospective medical case note review and parental recall using standardised questionnaires.
Setting: England and Wales.
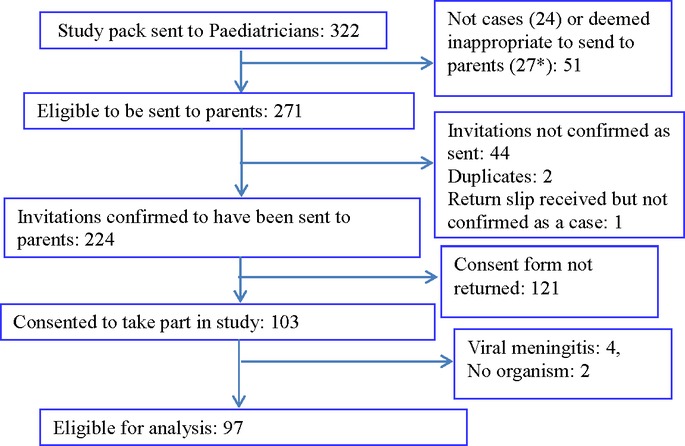
Participants: Infants aged <90 days with bacterial meningitis diagnosed between July 2010 and July 2013.
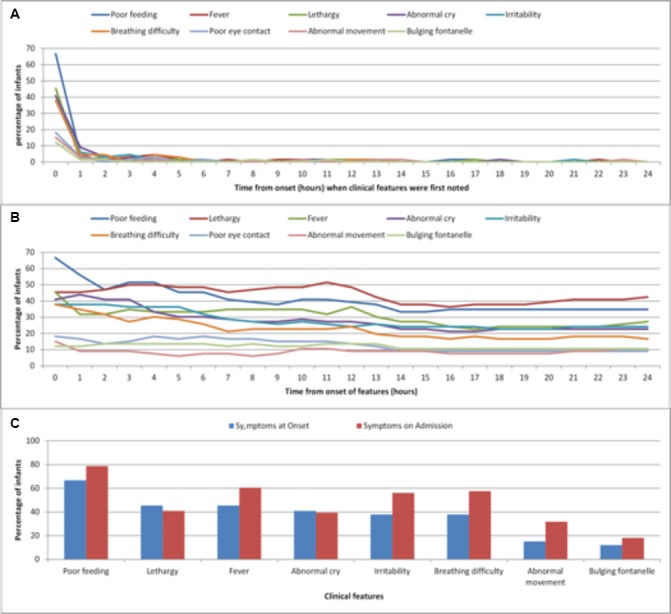
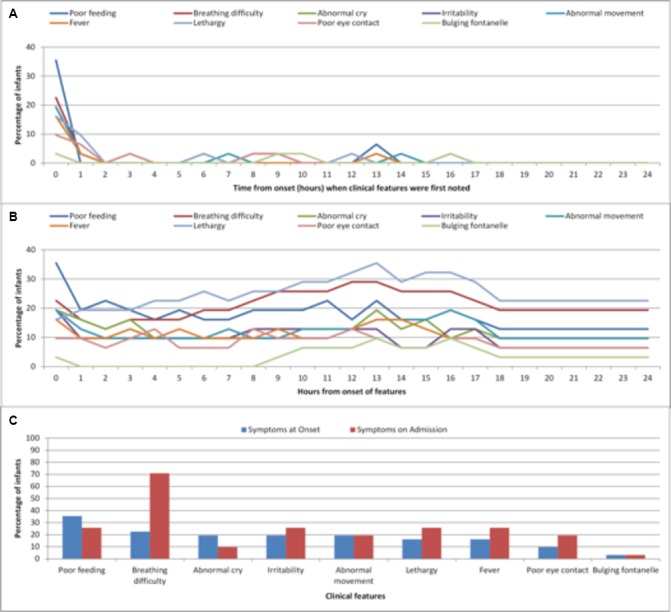
Results: Of the 97 cases recruited across England and Wales, 66 (68%) were admitted from home and 31 (32%) were in hospital prior to disease onset. Almost all symptoms reported by parents appeared at the onset of the illness, with very few new symptoms appearing subsequently. Overall, 20/66 (30%) infants were assessed to have received inappropriate prehospital management. The median time from onset of first symptoms to first help was 5 hours (IQR: 2-12) and from triage to receipt of first antibiotic dose was 2.0 hours (IQR: 1.0-3.3), significantly shorter in infants with fever or seizures at presentation compared with those without (1.7 (IQR: 1.0-3.0) vs 4.2 (IQR: 1.8-6.3) hours, p=0.02). Overall, 26 (39%) infants had a poor outcome in terms of death or neurological complication; seizures at presentation was the only significant independent risk factor (OR, 7.9; 95% CI 2.3 to 207.0). For cases in hospital already, the median time from onset to first dose of antibiotics was 2.6 (IQR: 1.3-9.8) hours, and 12/31 (39%) of infants had serious neurological sequelae at hospital discharge. Hearing test was not performed in 23% and when performed delayed by ≥4 weeks in 41%.
Conclusions: In young infants, the non-specific features associated with bacterial meningitis appear to show no progression from onset to admission, whereas there were small but significant differences in the proportion of infants with more specific symptoms at hospital admission compared with at the onset of the illness, highlighting the difficulties in early recognition by parents and healthcare professionals alike. A substantial proportion of infants received inappropriate prehospital and posthospital management. We propose a targeted campaign for education and harmonisation of practice with evidence-based management algorithms.
Keywords: assessment; bacterial; healthcare delivery; meningitis; young infants.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare no support from any organisation for the submitted work. PTH is a consultant for Novartis and Pfizer on group B streptococcus vaccines but receives no payment for this. NN is a consultant for Pfizer on meningococcal group B vaccines, and has received honoraria to teaching on meningitis from Novartis. All other authors declare no conflicts of interests. The ICMJE form for disclosure of potential conflicts of interest has been submitted.
Figures
References
-
- Okike IO, Johnson AP, Henderson KL, et al. Incidence, etiology, and outcome of bacterial meningitis in infants aged <90 days in the United kingdom and republic of Ireland: prospective, enhanced, national population-based surveillance. Clin Infect Dis 2014;59:e150–7. 10.1093/cid/ciu514 - DOI - PubMed
-
- Okike IO, Ladhani SN, Johnson AP, et al. Clinical characteristics and risk factors for poor outcomes in infants aged <90 days with bacterial meningitis in UK and Ireland. Pediatr Infect Dis J 2017. In Press. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases