

Pharmacokinetics, Tolerability, and Bacteriological Response of Rifampin Administered at 600, 900, and 1,200 Milligrams Daily in Patients with Pulmonary Tuberculosis
- PMID: 28827417
- PMCID: PMC5655063
- DOI: 10.1128/AAC.01054-17
Pharmacokinetics, Tolerability, and Bacteriological Response of Rifampin Administered at 600, 900, and 1,200 Milligrams Daily in Patients with Pulmonary Tuberculosis
Abstract
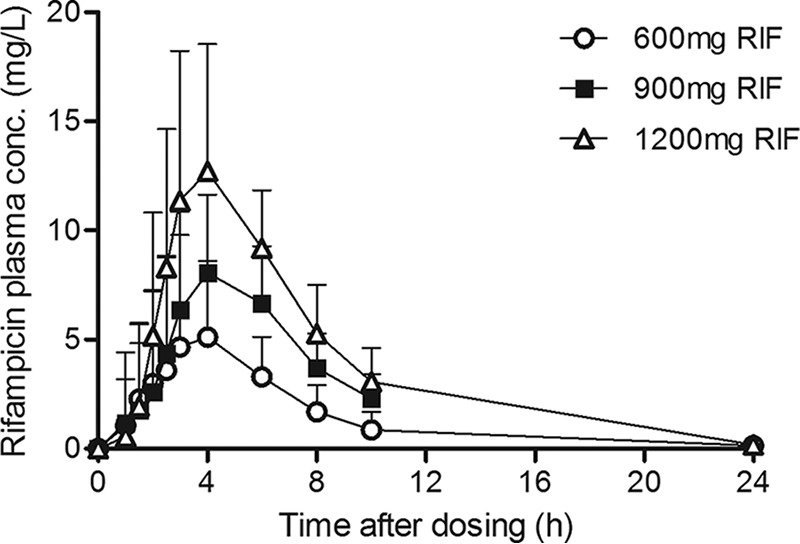
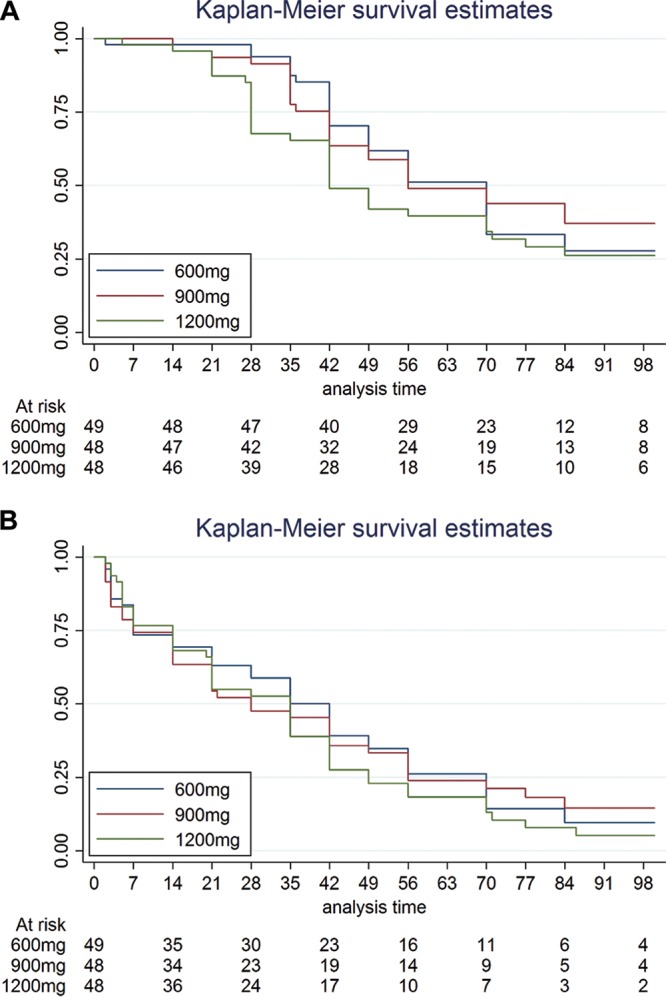
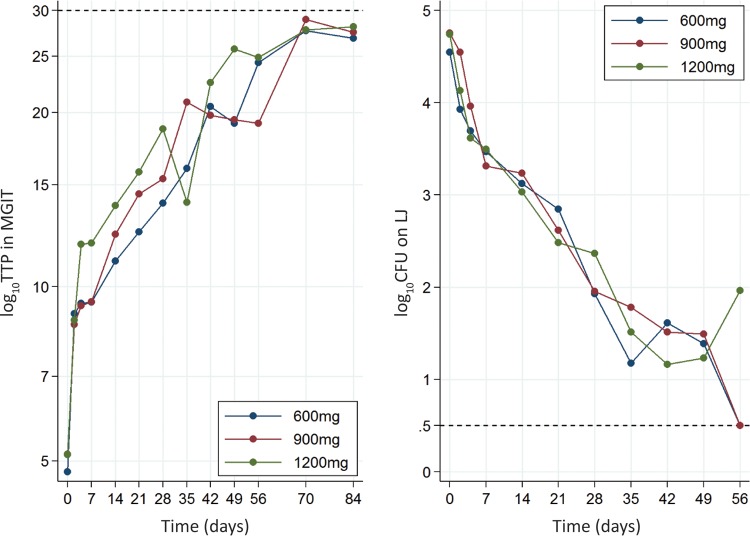
In a multiple-dose-ranging trial, we previously evaluated higher doses of rifampin in patients for 2 weeks. The objectives of the current study were to administer higher doses of rifampin for a longer period to compare the pharmacokinetics, safety/tolerability, and bacteriological activity of such regimens. In a double-blind, randomized, placebo-controlled, phase II clinical trial, 150 Tanzanian patients with tuberculosis (TB) were randomized to receive either 600 mg (approximately 10 mg/kg of body weight), 900 mg, or 1,200 mg rifampin combined with standard doses of isoniazid, pyrazinamide, and ethambutol administered daily for 2 months. Intensive pharmacokinetic sampling occurred in 63 patients after 6 weeks of treatment, and safety/tolerability was assessed. The bacteriological response was assessed by culture conversion in liquid and solid media. Geometric mean total exposures (area under the concentration-versus-time curve up to 24 h after the dose) were 24.6, 50.8, and 76.1 mg · h/liter in the 600-mg, 900-mg, and 1,200-mg groups, respectively, reflecting a nonlinear increase in exposure with the dose (P < 0.001). Grade 3 adverse events occurred in only 2 patients in the 600-mg arm, 4 patients in the 900-mg arm, and 5 patients in the 1,200-mg arm. No significant differences in the bacteriological response were observed. Higher daily doses of rifampin (900 and 1,200 mg) resulted in a more than proportional increase in rifampin exposure in plasma and were safe and well tolerated when combined with other first-line anti-TB drugs for 2 months, but they did not result in improved bacteriological responses in patients with pulmonary TB. These findings have warranted evaluation of even higher doses of rifampin in follow-up trials. (This study has been registered at ClinicalTrials.gov under identifier NCT00760149.).
Keywords: drug safety; pharmacokinetics; rifampin; tuberculosis.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- WHO. 2016. Global tuberculosis report 2016. WHO, Geneva, Switzerland: http://www.who.int/tb/publications/global_report/en/.
-
- Fox W, Ellard GA, Mitchison DA. 1999. Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946–1986, with relevant subsequent publications. Int J Tuberc Lung Dis 3(Suppl 2):S231–S279. - PubMed
-
- Jayaram R, Gaonkar S, Kaur P, Suresh BL, Mahesh BN, Jayashree R, Nandi V, Bharat S, Shandil RK, Kantharaj E, Balasubramanian V. 2003. Pharmacokinetics-pharmacodynamics of rifampin in an aerosol infection model of tuberculosis. Antimicrob Agents Chemother 47:2118–2124. doi: 10.1128/AAC.47.7.2118-2124.2003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
