

Local and systemic immunomodulatory mechanisms triggered by Human Papillomavirus transformed cells: a potential role for G-CSF and neutrophils
- PMID: 28827632
- PMCID: PMC5566396
- DOI: 10.1038/s41598-017-09079-3
Local and systemic immunomodulatory mechanisms triggered by Human Papillomavirus transformed cells: a potential role for G-CSF and neutrophils
Abstract
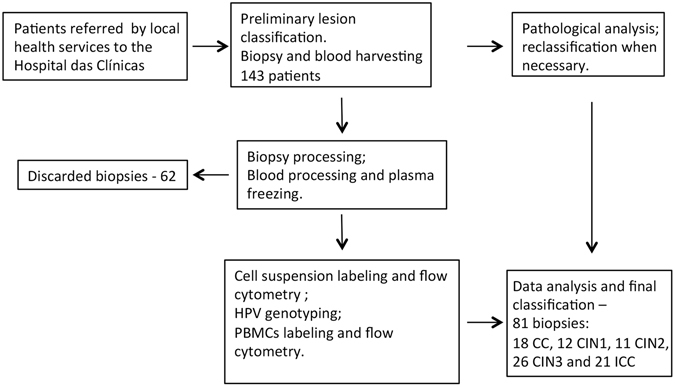
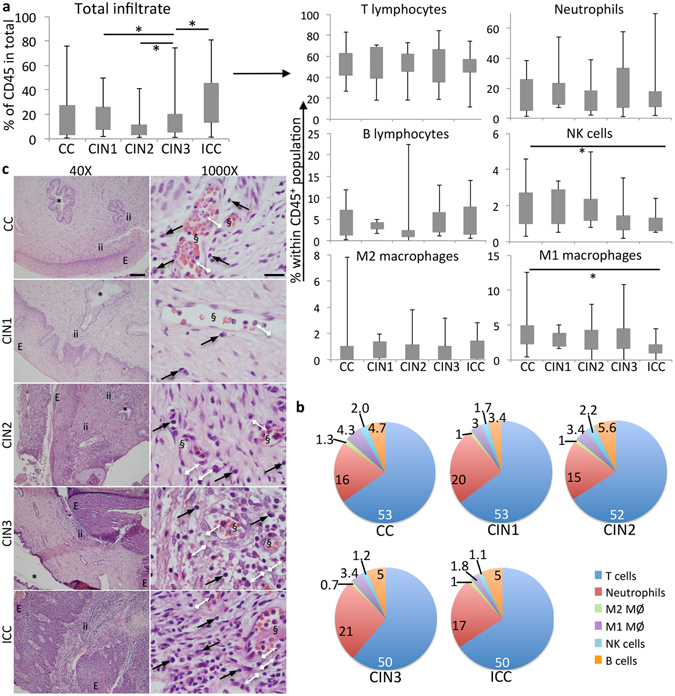
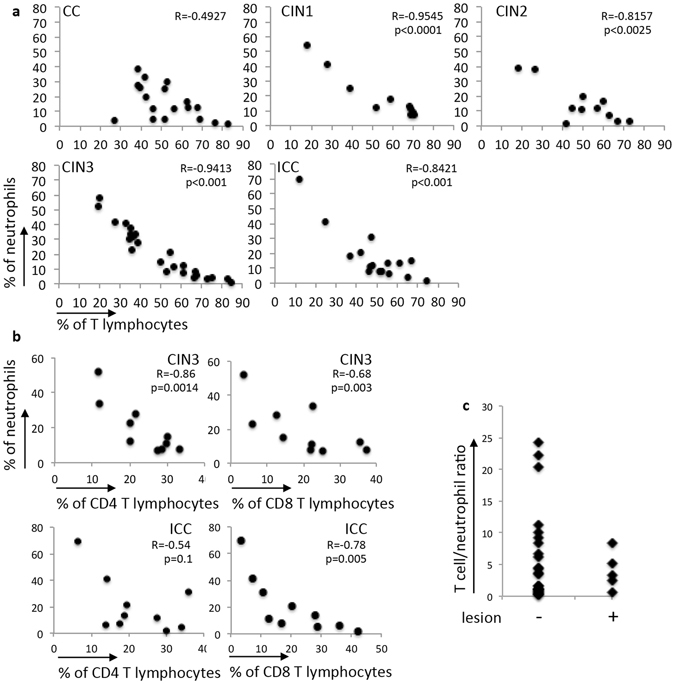
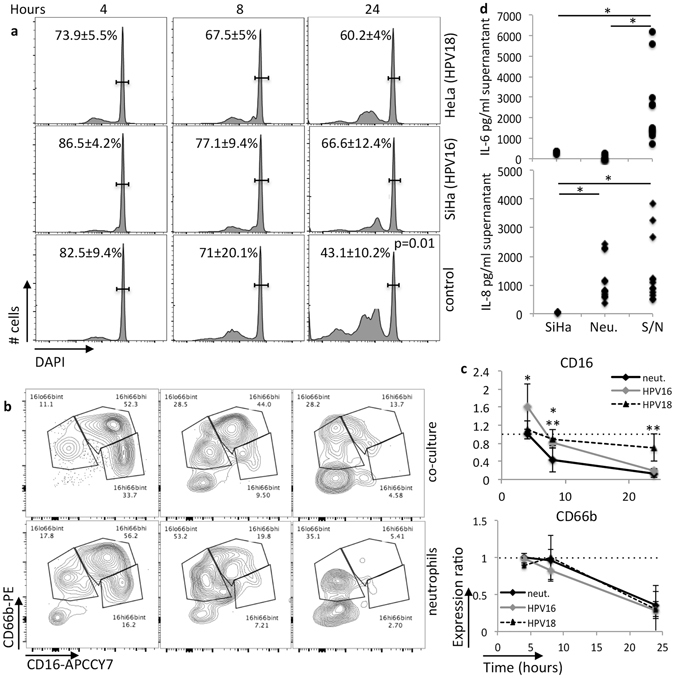
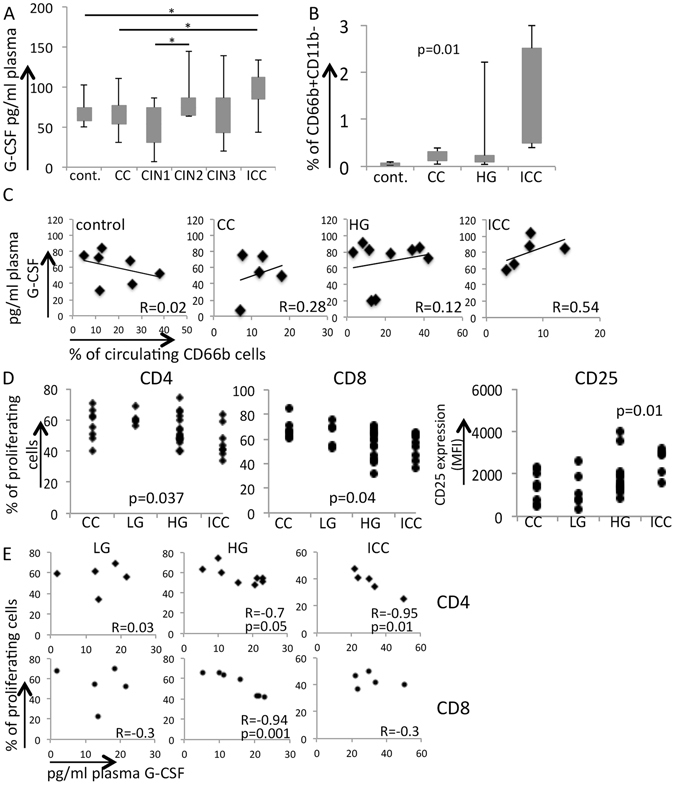
Cervical cancer is the last stage of a series of molecular and cellular alterations initiated with Human Papillomavirus (HPV) infection. The process involves immune responses and evasion mechanisms, which culminates with tolerance toward tumor antigens. Our objective was to understand local and systemic changes in the interactions between HPV associated cervical lesions and the immune system as lesions progress to cancer. Locally, we observed higher cervical leukocyte infiltrate, reflected by the increase in the frequency of T lymphocytes, neutrophils and M2 macrophages, in cancer patients. We observed a strong negative correlation between the frequency of neutrophils and T cells in precursor and cancer samples, but not cervicitis. In 3D tumor cell cultures, neutrophils inhibited T cell activity, displayed longer viability and longer CD16 expression half-life than neat neutrophil cultures. Systemically, we observed higher plasma G-CSF concentration, higher frequency of immature low density neutrophils, and tolerogenic monocyte derived dendritic cells, MoDCs, also in cancer patients. Interestingly, there was a negative correlation between T cell activation by MoDCs and G-CSF concentration in the plasma. Our results indicate that neutrophils and G-CSF may be part of the immune escape mechanisms triggered by cervical cancer cells, locally and systemically, respectively.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
