

Transpulmonary pressure: importance and limits
- PMID: 28828360
- PMCID: PMC5537111
- DOI: 10.21037/atm.2017.07.22
Transpulmonary pressure: importance and limits
Abstract
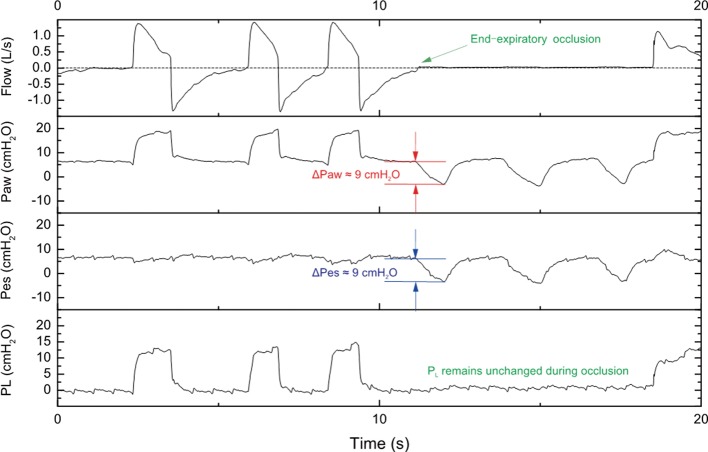
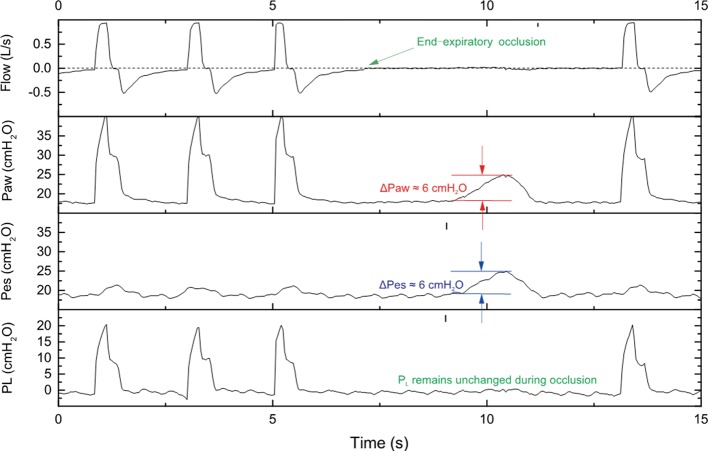
Transpulmonary pressure (PL) is computed as the difference between airway pressure and pleural pressure and separates the pressure delivered to the lung from the one acting on chest wall and abdomen. Pleural pressure is measured as esophageal pressure (PES) through dedicated catheters provided with esophageal balloons. We discuss the role of PL in assessing the effects of mechanical ventilation in patients with acute respiratory distress syndrome (ARDS). In the supine position, directly measured PL represents the pressure acting on the alveoli and airways. Because there is a pressure gradient in the pleural space from the non-dependent to the dependent zones, the pressure in the esophagus probably represents the pressure at a mid-level between sternal and vertebral regions. For this reason, it has been proposed to set the end-expiratory pressure in order to get a positive value of PL. This improves oxygenation and compliance. PL can also be estimated from airway pressure plateau and the ratio of lung to respiratory elastance (elastance-derived method). Some data suggest that this latter calculation may better estimate PL in the nondependent lung zones, at risk for hyperinflation. Elastance-derived PL at end-inspiration (PLend-insp) may be a good surrogate of end-inspiratory lung stress for the "baby lung", at least in non-obese patients. Limiting end-inspiratory PL to 20-25 cmH2O appears physiologically sound to mitigate ventilator-induced lung injury (VILI). Last, lung driving pressure (∆PL) reflects the tidal distending pressure. Changes in PL may also be assessed during assisted breathing to take into account the additive effects of spontaneous breathing and mechanical breaths on lung distension. In summary, despite limitations, assessment of PL allows a deeper understanding of the risk of VILI and may potentially help tailor ventilator settings.
Keywords: Acute respiratory distress syndrome (ARDS); driving pressure; esophageal pressure (PES); mechanical ventilation; respiratory mechanics; ventilator-induced lung injury (VILI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical