

Spontaneous breathing: a double-edged sword to handle with care
- PMID: 28828367
- PMCID: PMC5537122
- DOI: 10.21037/atm.2017.06.55
Spontaneous breathing: a double-edged sword to handle with care
Abstract
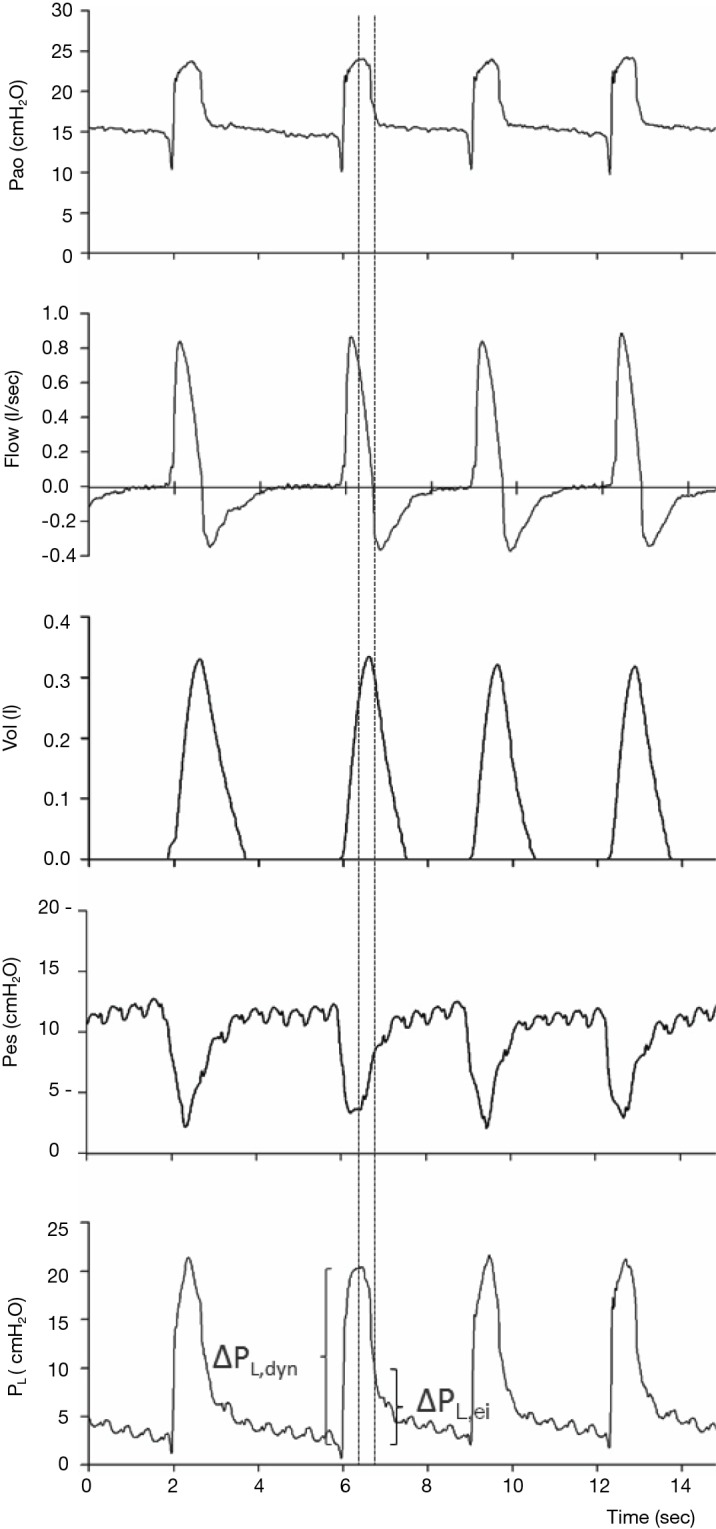
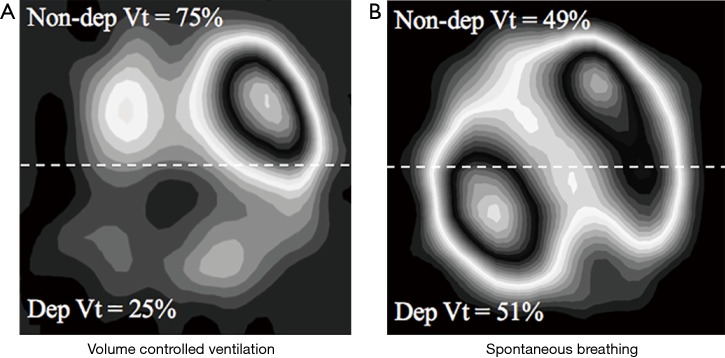
In acute hypoxemic respiratory failure (AHRF) and acute respiratory distress syndrome (ARDS) patients, spontaneous breathing is associated with multiple physiologic benefits: it prevents muscles atrophy, avoids paralysis, decreases sedation needs and is associated with improved hemodynamics. On the other hand, in the presence of uncontrolled inspiratory effort, severe lung injury and asynchronies, spontaneous ventilation might also worsen lung edema, induce diaphragm dysfunction and lead to muscles exhaustion and prolonged weaning. In the present review article, we present physiologic mechanisms driving spontaneous breathing, with emphasis on how to implement basic and advanced respiratory monitoring to assess lung protection during spontaneous assisted ventilation. Then, key benefits and risks associated with spontaneous ventilation are described. Finally, we propose some clinical means to promote protective spontaneous breathing at the bedside. In summary, early switch to spontaneous assisted breathing of acutely hypoxemic patients is more respectful of physiology and might yield several advantages. Nonetheless, risk of additional lung injury is not completely avoided during spontaneous breathing and careful monitoring of target physiologic variables such as tidal volume (Vt) and driving transpulmonary pressure should be applied routinely. In clinical practice, multiple interventions such as extracorporeal CO2 removal exist to maintain inspiratory effort, Vt and driving transpulmonary pressure within safe limits but more studies are needed to assess their long-term efficacy.
Keywords: Spontaneous breathing; acute respiratory distress syndrome (ARDS); esophageal pressure (Pes); physiology; ventilator-induced lung injury (VILI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Dot I, Pérez-Teran P, Samper MA, et al. Diaphragm Dysfunction in Mechanically Ventilated Patients. Arch Bronconeumol 2017;53:150-6. - PubMed
-
- Levine S, Nguyen T, Taylor N, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med 2008;358:1327-35. - PubMed
-
- Demoule A, Clavel M, Rolland-Debord C, et al. Neurally adjusted ventilatory assist as an alternative to pressure support ventilation in adults: a French multicentre randomized trial. Intensive Care Med 2016;42:1723-32. - PubMed
-
- Bellani G, Laffey JG, Pham T, et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016;315:788-800. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical