

Right heart function during acute respiratory distress syndrome
- PMID: 28828370
- PMCID: PMC5537114
- DOI: 10.21037/atm.2017.06.66
Right heart function during acute respiratory distress syndrome
Abstract
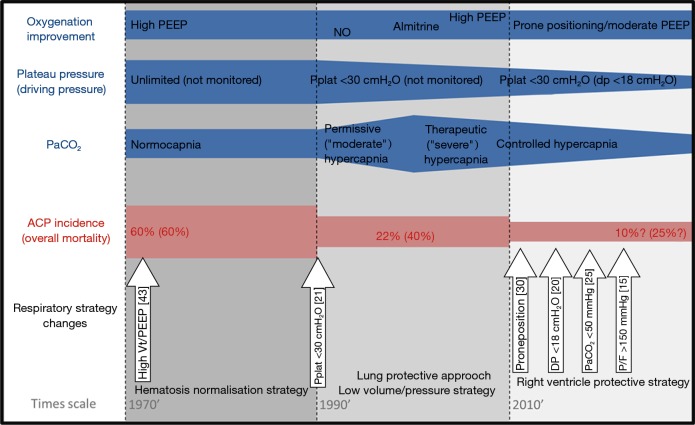
Acute respiratory distress syndrome (ARDS) is burdened with significant mortality, mainly in connection with circulatory failure. The right ventricle (RV) is the weak link of hemodynamic stability among ARDS patients and its failure, also named "severe" acute cor pulmonale (ACP), is responsible for excess mortality. Driving pressure ≥18 cmH2O, PaCO2 ≥48 mmHg and PaO2/FiO2 <150 mmHg are three preventable factors recently identified as independently associated with ACP, on which ventilator strategy designed to protect the RV has to focus. This is largely achieved by the use of early and extended sessions of prone positioning (PP) and by daily monitoring of the RV by echocardiography.
Keywords: Acute respiratory distress syndrome (ARDS); acute cor pulmonale (ACP); driving pressure; hypercapnia; oxygenation; right ventricle (RV).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Vieillard-Baron A, Girou E, Valente E, et al. Predictors of mortality in acute respiratory distress syndrome. Focus On the role of right heart catheterization. Am J Respir Crit Care Med 2000;161:1597-601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous