

Growth and weight gain in children with juvenile idiopathic arthritis: results from the ReACCh-Out cohort
- PMID: 28830457
- PMCID: PMC5567720
- DOI: 10.1186/s12969-017-0196-7
Growth and weight gain in children with juvenile idiopathic arthritis: results from the ReACCh-Out cohort
Abstract
Background: With modern treatments, the effect of juvenile idiopathic arthritis (JIA) on growth may be less than previously reported. Our objective was to describe height, weight and body mass index (BMI) development in a contemporary JIA inception cohort.
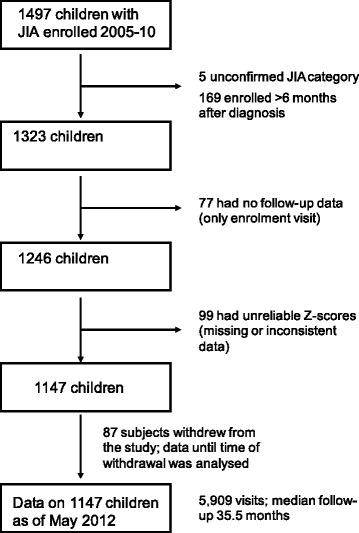
Methods: Canadian children newly-diagnosed with JIA 2005-2010 had weight and height measurements every 6 months for 2 years, then yearly up to 5 years. These measurements were used to calculate mean age- and sex-standardized Z-scores, and estimate prevalence and cumulative incidence of growth impairments, and the impact of disease activity and corticosteroids on growth.
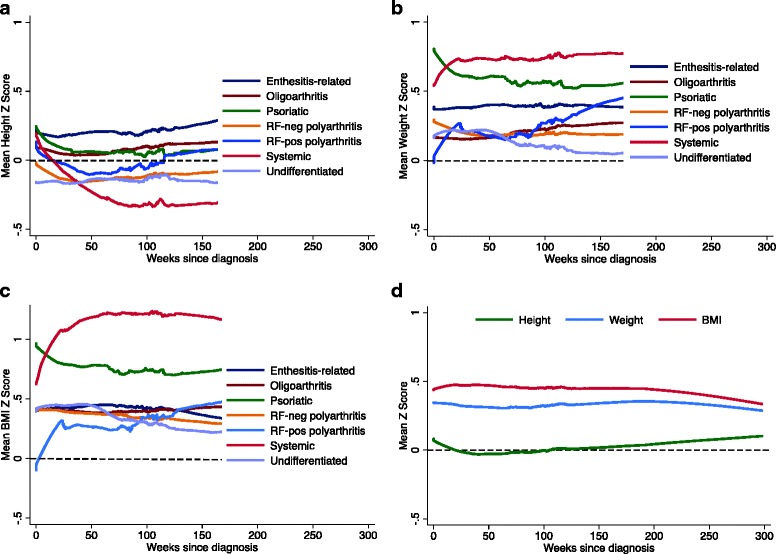
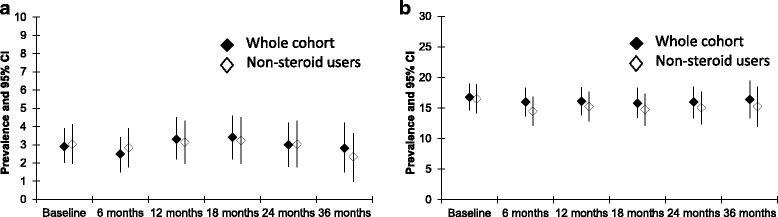
Results: One thousand one hundred forty seven children were followed for median 35.5 months. Mean Z-scores, and the point prevalence of short stature (height < 2.5th percentile, 2.5% to 3.4%) and obesity (BMI > 95th percentile, 15.8% to 16.4%) remained unchanged in the whole cohort. Thirty-three children (2.9%) developed new-onset short stature, while 27 (2.4%) developed tall stature (>97.5th percentile). Children with systemic arthritis (n = 77) had an estimated 3-year cumulative incidence of 9.3% (95%CI: 4.3-19.7) for new-onset short stature and 34.4% (23-49.4) for obesity. Most children (81.7%) received no systemic corticosteroids, but 1 mg/Kg/day prednisone-equivalent maintained for 6 months corresponded to a drop of 0.64 height Z-scores (0.56-0.82) and an increase of 0.74 BMI Z-scores (0.56-0.92). An increase of 1 in the 10-cm physician global assessment of disease activity maintained for 6 months corresponded to a drop of 0.01 height Z-scores (0-0.02).
Conclusions: Most children in this modern JIA cohort grew and gained weight as children in the general population. About 1 in 10 children who had systemic arthritis, uncontrolled disease and/or prolonged corticosteroid use, had increased risk of growth impairment.
Keywords: Corticosteroids; Growth; Juvenile arthritis; Obesity.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by research ethics boards at each participating institution. Parents provided informed written consent, and patients provided assent where appropriate.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Figures
References
-
- Petty RE, Southwood TR, Manners P, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol2004;31(2):390–2. - PubMed
-
- Guzman J, Oen K, Tucker LB, Huber AM, Shiff N, Boire G, Scuccimarri R, Berard R, Tse SM, Morishita K, Stringer E, Johnson N, Levy DM, Duffy KW, Cabral DA, Rosenberg AM, Larché M, Dancey P, Petty RE, Laxer RM, Silverman E, Miettunen P, Chetaille AL, Haddad E, Houghton K, Spiegel L, Turvey SE, Schmeling H, Lang B, Ellsworth J, Ramsey S, Bruns A, Campillo S, Benseler S, Chédeville G, Schneider R, Yeung R, Duffy CM, for the ReACCh-Out investigators The outcomes of juvenile idiopathic arthritis in children managed with contemporary treatments: results from the ReACCh-Out cohort. Ann Rheum Dis. 2015;74(10):1854–1860. doi: 10.1136/annrheumdis-2014-205372. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
