

Survival outcomes of hepatectomy for stage B Hepatocellular carcinoma in the BCLC classification
- PMID: 28830473
- PMCID: PMC5568344
- DOI: 10.1186/s12957-017-1229-x
Survival outcomes of hepatectomy for stage B Hepatocellular carcinoma in the BCLC classification
Abstract
Background: Because hepatectomy is not recommended in patients with stage B hepatocellular carcinoma (HCC) of the Barcelona Clinic Liver Cancer (BCLC) staging, we evaluated the survival outcomes of hepatectomy for stage B in the BCLC system.
Methods: Data were collected from 297 consecutive adult stage B patients who underwent curative hepatectomy for HCC between 1996 and 2014 in Hokkaido University Hospital. Overall survival (OS), disease-free survival (DFS), and risk factors were analyzed using the Kaplan-Meier method. Independent prognostic factors were evaluated using a Cox proportional hazards regression model. AP-factor (alpha-fetoprotein [AFP] × protein induced by vitamin K absence or antagonism factor II [PIVKA-II]) was categorized according to the serum concentrations of AFP and PIVKA-II: AP1 (AFP < 200 ng/ml and PIVKA-II < 100 mAU/ml), AP2 (AFP × PIVKA-II < 105), and AP3 (AFP × PIVKA-II ≥ 105).
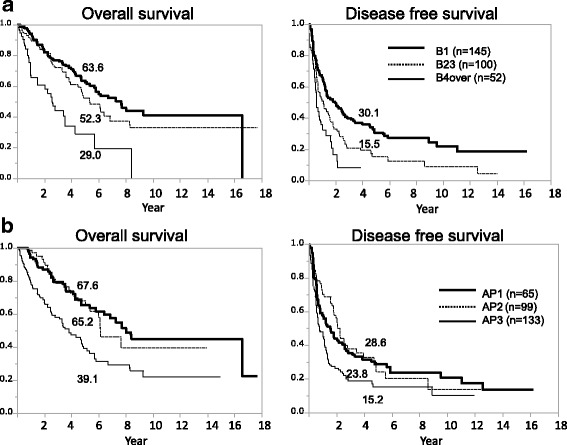
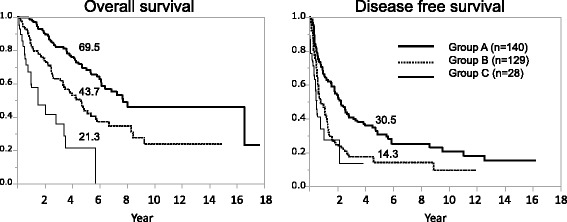
Results: There were 130 deaths among our 297 stage B patients (43.8%). The causes of death in these cases were HCC recurrence (n = 106; 81.5%), liver failure (n = 7; 5.4%), and other causes (n = 17; 16.1%). The operative mortality rate was 0.34% (1/297). The 5-year OS and DFS rates for the stage B cases were 54.3 and 21.9%, respectively. By multivariate analysis, tumor number and AP-factor were risk factors for both survival and recurrence that were tumor related and could be evaluated preoperatively. The study patients with stage B HCC were classified into three groups by tumor number (B1, 1; B23, 2 or 3; B4over: ≥4) and into three groups stratified by AP-factor (AP1, AP2, and AP3). The 5-year OS rates of B1, B23, and B4over were 63.6, 52.3, and 29.0%. The 5-year OS rates of AP1, AP2, and AP3 were 67.6, 65.2, and 39.1%. Stratified by the 5-year OS rate, stage B HCC patients were classified into three subgroups (A-C).The 5-year OS rates of groups A (B1 or B23 and AP-1 or AP-2), B (B1 or B23 and AP-3, or B4over and AP-1 or AP-2), and C (B4over and AP-3) were 69.5, 43.7, and 21.3%.
Conclusion: Stage B HCC patients with a tumor number ≤ 3 and/or AP-factor < 1 × 105 show acceptable 5-year OS rates and could be treated by hepatectomy.
Keywords: BCLC staging.; Hepatectomy; Hepatocellar carcinoma.
Conflict of interest statement
Ethics approval and consent to participate
All analyses in our present study were performed in accordance with the ethical guidelines of Hokkaido University Hospital. This study was approved by the Institutional Review Board of Hokkaido University. The study was performed according to the Helsinki Declaration guidelines.
Consent for publication
We obtained consent for publication from the patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Arii S, Yamaoka Y, Futagawa S, Inoue K, Kobayashi K, Kojiro M, Makuuchi M, Nakamura Y, Okita K, Yamada R. Results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in Japan. The liver cancer study Group of Japan. Hepatology. 2000;32(6):1224–1229. doi: 10.1053/jhep.2000.20456. - DOI - PubMed
-
- Kudo M, Izumi N, Kokudo N, Matsui O, Sakamoto M, Nakashima O, Kojiro M, Makuuchi M, Hepatology HCCEPoJSo Management of hepatocellular carcinoma in Japan: consensus-based clinical practice guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated version. Dig Dis. 2011;29(3):339–364. doi: 10.1159/000327577. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
