

An economic evaluation of the healthcare cost of tinnitus management in the UK
- PMID: 28830503
- PMCID: PMC5567641
- DOI: 10.1186/s12913-017-2527-2
An economic evaluation of the healthcare cost of tinnitus management in the UK
Abstract
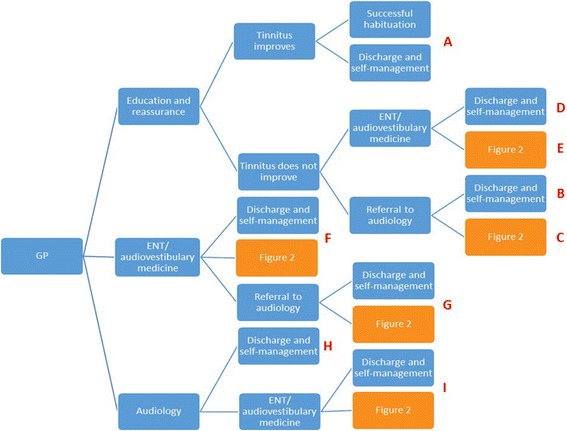
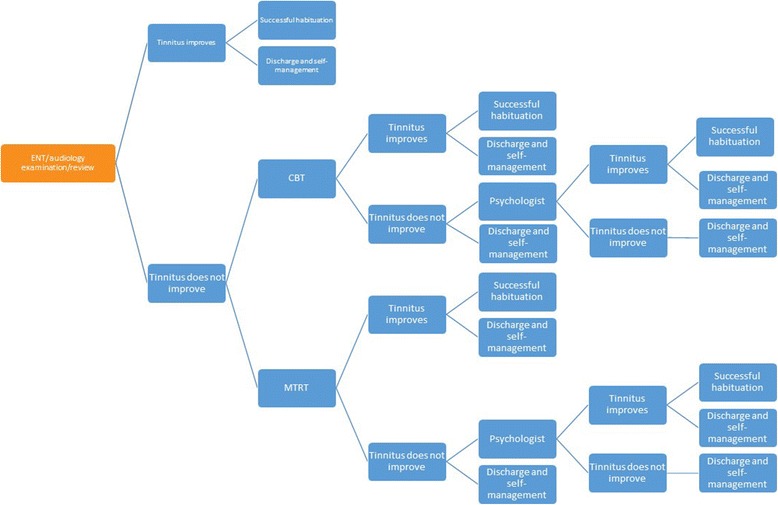
Background: There is no standard treatment pathway for tinnitus patients in the UK. Possible therapies include education and reassurance, cognitive behavioural therapies, modified tinnitus retraining therapy (education and sound enrichment), or amplification of external sound using hearing aids. However, the effectiveness of most therapies is somewhat controversial. As health services come under economic pressure to deploy resources more effectively there is an increasing need to demonstrate the value of tinnitus therapies, and how value may be continuously enhanced. The objective of this project was to map out existing clinical practice, estimate the NHS costs associated with the management approaches used, and obtain initial indicative estimates of cost-effectiveness.
Methods: Current treatment pathways, costs and health outcomes were determined from the tinnitus literature, national statistics, a patient survey, and expert opinion. These were used to create an Excel-based economic model of therapy options for tinnitus patients. The probabilities associated with the likelihood of an individual patient receiving a particular combination of therapies was used to calculate the average cost of treatment per patient, average health outcome per patient measured in QALYs gained, and cost-effectiveness, measured by the average cost per QALY gained.
Results: The average cost of tinnitus treatment per patient per year is GB£717, equating to an NHS healthcare bill of GB£750 million per year. Across all pathways, tinnitus therapy costs £10,600 per QALY gained. Results were relatively insensitive to restrictions on access to cognitive behaviour therapy, and a subsequent reliance on other therapies.
Conclusions: NHS provisions for tinnitus are cost-effective against the National Institute for Health and Care Excellence cost-effective threshold. Most interventions help, but education alone offers very small QALY gains. The most cost-effective therapies in the model were delivered within audiology.
Keywords: Audiology; Clinical psychology; Cognitive behaviour therapy; Cost effectiveness; Ear nose and throat; General practice; Hearing aids; Tinnitus.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable. Data based project.
Consent for publication
Not applicable.
Competing interests
CP and PB had support from the British Tinnitus Association for the submitted work. DM is a Trustee of the British Tinnitus Association; DJH and TK are chair and member respectively of the British Society of Audiology Tinnitus and Hyperacusis Special Interest Group.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
