

Expression and Clinical Significance of ILF2 in Gastric Cancer
- PMID: 28831206
- PMCID: PMC5555027
- DOI: 10.1155/2017/4387081
Expression and Clinical Significance of ILF2 in Gastric Cancer
Abstract
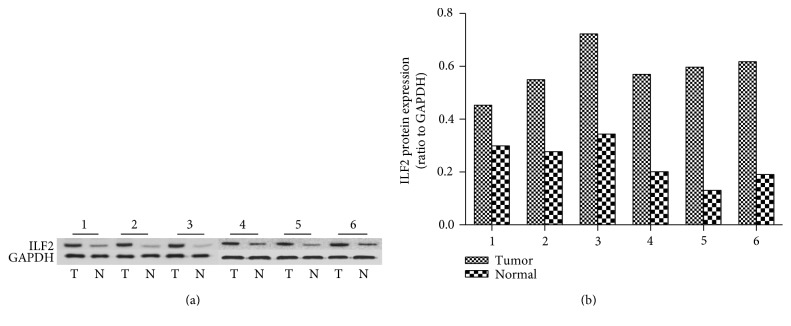
The aim of this study is to investigate the expression levels and clinical significance of ILF2 in gastric cancer. The mRNA and protein expression levels of ILF2 were, respectively, examined by quantitative real-time PCR (qRT-PCR) and Western blot from 21 paired fresh frozen GC tissues and corresponding normal gastric tissues. In order to analyze the expression pattern of ILF2 in GC, 60 paired paraffin-embedded GC slides and corresponding normal gastric slides were detected by immunohistochemistry (IHC) assay. The correlation between ILF2 protein expression levels and clinicopathological parameters, overall survival (OS), disease-free survival (DFS), and clinical prognosis were analyzed by statistical methods. Significantly higher levels of ILF2 were detected in GC tissues compared with normal controls at both mRNA and protein level. High expression of ILF2 was tightly correlated with depth of invasion, lymph node metastasis, pathological stage, and histological differentiation. Log-rank test showed that high expression of ILF2 was positively associated with poor clinical prognosis. Multivariate analysis identified that ILF2 was an independent prognostic factor for OS and DFS. Our findings suggest that ILF2 may be a valuable biomarker and a novel potential prognosis predictor for GC patients.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
