

Evaluation of Inflammatory Markers in a Large Sample of Obstructive Sleep Apnea Patients without Comorbidities
- PMID: 28831208
- PMCID: PMC5555019
- DOI: 10.1155/2017/4573756
Evaluation of Inflammatory Markers in a Large Sample of Obstructive Sleep Apnea Patients without Comorbidities
Abstract
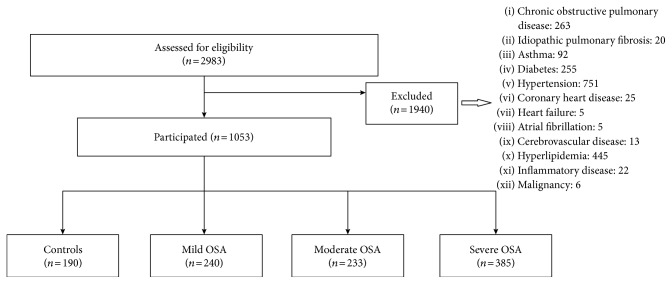
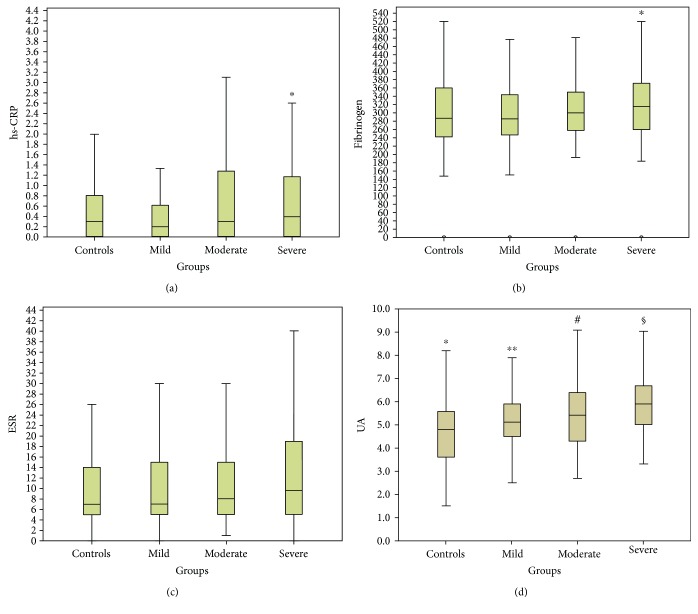
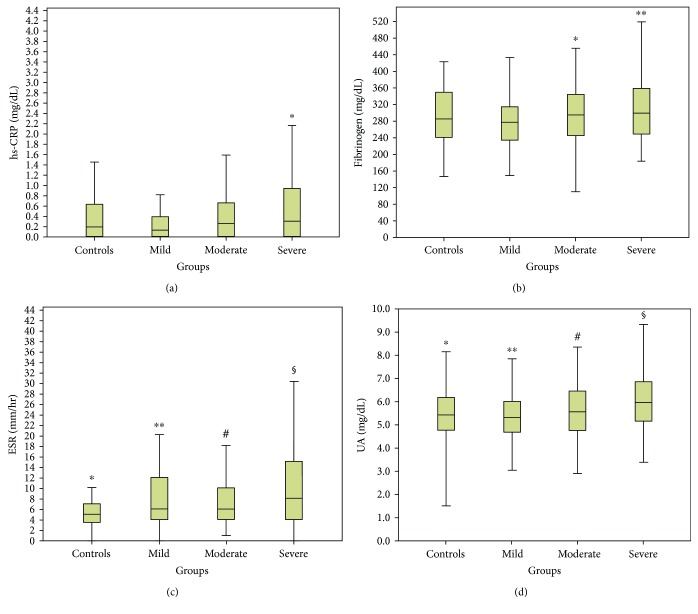
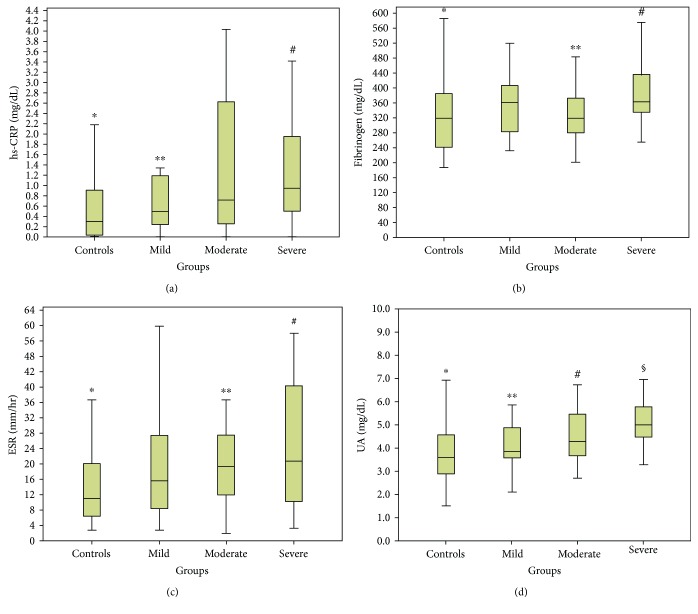
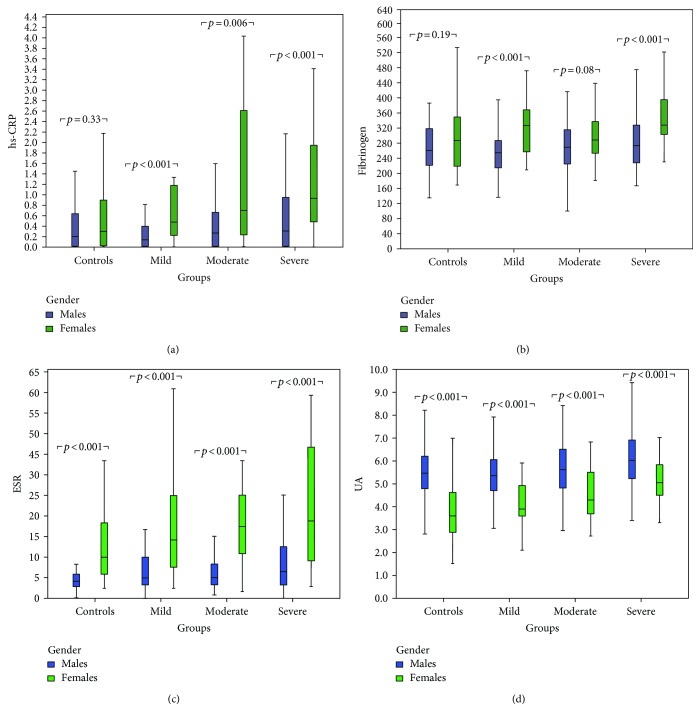
Systemic inflammation is important in obstructive sleep apnea (OSA) pathophysiology and its comorbidity. We aimed to assess the levels of inflammatory biomarkers in a large sample of OSA patients and to investigate any correlation between these biomarkers with clinical and polysomnographic (PSG) parameters. This was a cross-sectional study in which 2983 patients who had undergone a polysomnography for OSA diagnosis were recruited. Patients with known comorbidities were excluded. Included patients (n = 1053) were grouped according to apnea-hypopnea index (AHI) as mild, moderate, and severe. Patients with AHI < 5 served as controls. Demographics, PSG data, and levels of high-sensitivity C-reactive protein (hs-CRP), fibrinogen, erythrocyte sedimentation rate (ESR), and uric acid (UA) were measured and compared between groups. A significant difference was found between groups in hs-CRP, fibrinogen, and UA. All biomarkers were independently associated with OSA severity and gender (p < 0.05). Females had increased levels of hs-CRP, fibrinogen, and ESR (p < 0.001) compared to men. In contrast, UA levels were higher in men (p < 0.001). Our results suggest that inflammatory markers significantly increase in patients with OSA without known comorbidities and correlate with OSA severity. These findings may have important implications regarding OSA diagnosis, monitoring, treatment, and prognosis. This trial is registered with ClinicalTrials.gov number NCT03070769.
Figures
Similar articles
-
Erythrocyte sedimentation rate may help predict severity of obstructive sleep apnea.Sleep Breath. 2016 Mar;20(1):419-24. doi: 10.1007/s11325-015-1245-4. Epub 2015 Aug 28. Sleep Breath. 2016. PMID: 26315467
-
Influence of gender on C-reactive protein, fibrinogen, and erythrocyte sedimentation rate in obstructive sleep apnea.Antiinflamm Antiallergy Agents Med Chem. 2014 Mar;13(1):56-63. doi: 10.2174/18715230113129990015. Antiinflamm Antiallergy Agents Med Chem. 2014. PMID: 23862972
-
Structural and serum surrogate markers of cerebrovascular disease in obstructive sleep apnea (OSA): association of mild OSA with early atherosclerosis.J Neurol. 2006 Jun;253(6):746-52. doi: 10.1007/s00415-006-0110-6. Epub 2006 Mar 6. J Neurol. 2006. PMID: 16511651
-
Is C-reactive protein a marker of obstructive sleep apnea?: A meta-analysis.Medicine (Baltimore). 2017 May;96(19):e6850. doi: 10.1097/MD.0000000000006850. Medicine (Baltimore). 2017. PMID: 28489776 Free PMC article. Review.
-
Effect of Sleep Surgery on C-Reactive Protein Levels in Adults With Obstructive Sleep Apnea: A Meta-Analysis.Laryngoscope. 2021 May;131(5):1180-1187. doi: 10.1002/lary.29212. Epub 2020 Oct 28. Laryngoscope. 2021. PMID: 33111981 Review.
Cited by
-
Relationship between monocyte to HDL cholesterol ratio and concomitant cardiovascular disease in Chinese Han patients with obstructive sleep apnea.Cardiovasc Diagn Ther. 2019 Aug;9(4):362-370. doi: 10.21037/cdt.2019.08.02. Cardiovasc Diagn Ther. 2019. PMID: 31555541 Free PMC article.
-
Continuous positive airway pressure therapy suppresses inflammatory cytokines and improves glucocorticoid responsiveness in patients with obstructive sleep apnea and asthma: A case-control study.Ann Thorac Med. 2022 Jul-Sep;17(3):166-172. doi: 10.4103/atm.atm_37_22. Epub 2022 Jul 9. Ann Thorac Med. 2022. PMID: 35968397 Free PMC article.
-
Precision multiparameter tracking of inflammation on timescales of hours to years using serial dried blood spots.Bioanalysis. 2020 Jul;12(13):937-955. doi: 10.4155/bio-2019-0278. Epub 2020 Apr 7. Bioanalysis. 2020. PMID: 32253915 Free PMC article.
-
Androgens modulate chronic intermittent hypoxia effects on brain and behavior.Horm Behav. 2018 Nov;106:62-73. doi: 10.1016/j.yhbeh.2018.09.005. Epub 2018 Oct 6. Horm Behav. 2018. PMID: 30268884 Free PMC article.
-
Sleep Behaviour in Sickle Cell Disease: A Systematic Review and Meta-Analysis.Children (Basel). 2024 Dec 26;12(1):21. doi: 10.3390/children12010021. Children (Basel). 2024. PMID: 39857852 Free PMC article. Review.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
