

Microfocused Ultrasound with Visualization and Calcium Hydroxylapatite for Improving Skin Laxity and Cellulite Appearance
- PMID: 28831339
- PMCID: PMC5548562
- DOI: 10.1097/GOX.0000000000001388
Microfocused Ultrasound with Visualization and Calcium Hydroxylapatite for Improving Skin Laxity and Cellulite Appearance
Abstract
Age-associated skin laxity contributes to worsening of cellulite appearance. This study evaluated the effects of microfocused ultrasound with visualization (MFU-V; Ultherapy) in combination with diluted calcium hydroxylapatite (CaHA; Radiesse) on cellulite appearance and on neocollagenesis.
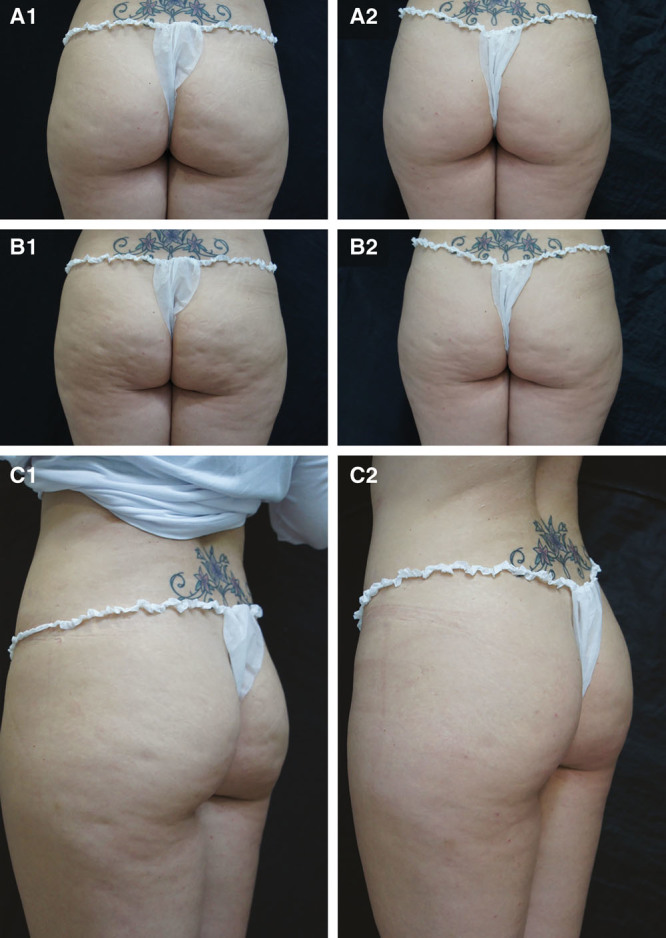
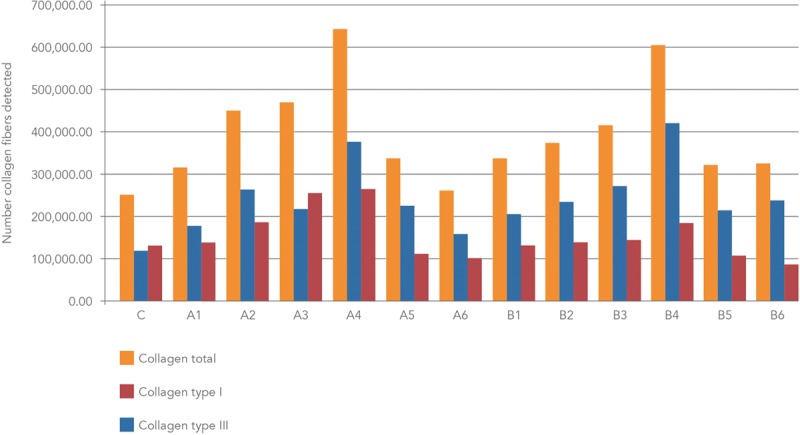
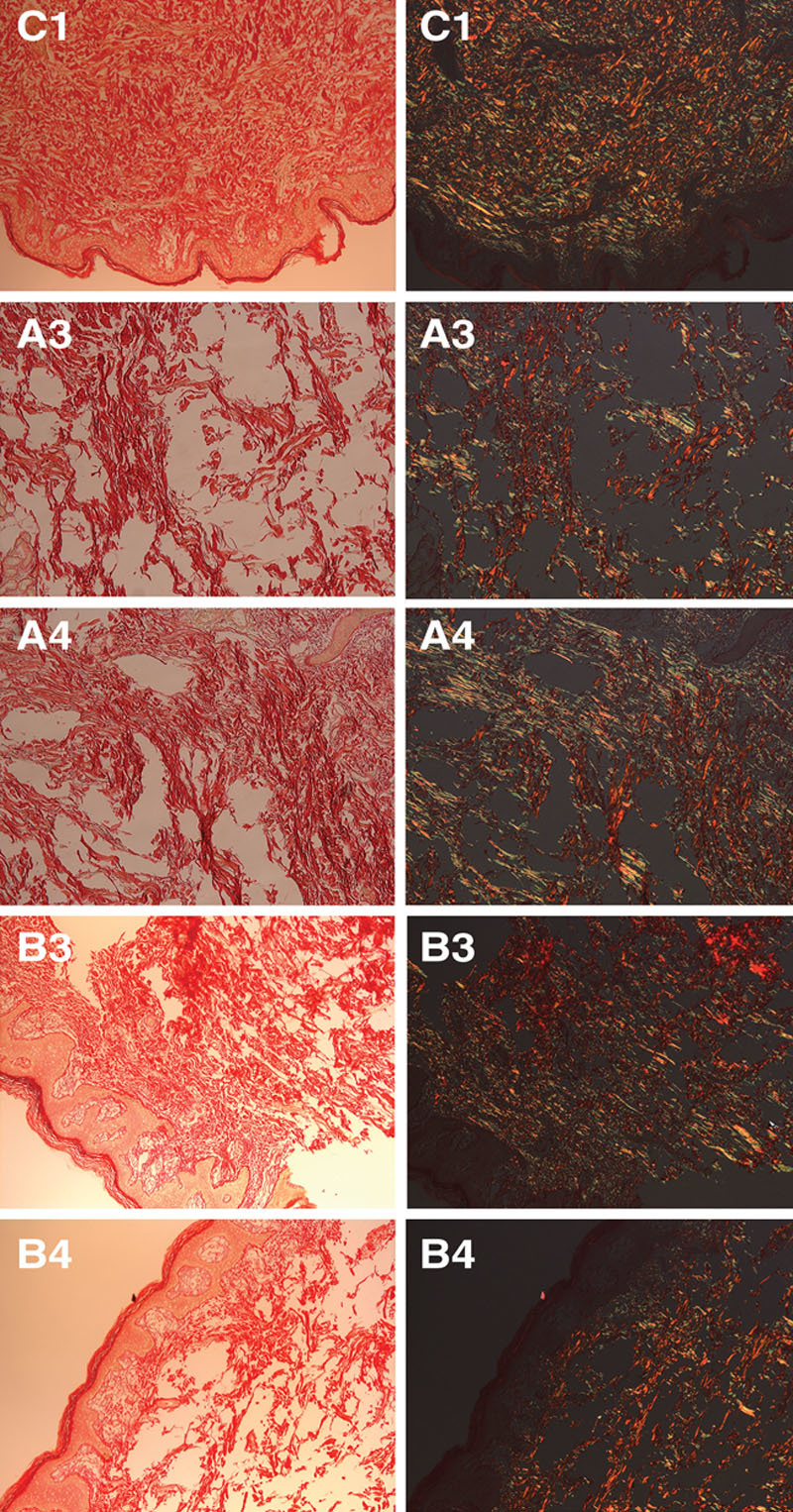
Methods: Twenty women (18-55 years old) with skin laxity and moderate-to-severe cellulite on the buttocks and thighs were retrospectively enrolled. MFU-V was applied using 4 and 7 MHz transducers (25 lines/transducer/site) and immediately followed by subdermal CaHA injection (1 ml/buttock or thigh). Photographs at baseline and 90 days were assessed by 2 independent, blinded evaluators using a 5-item cellulite severity scale. One subject scheduled for thighplasty received treatment with 6 different CaHA dilutions (0.3 ml/5 cm2) followed by MFU-V. Tissue specimens from each dilution site were examined under polarized light microscopy to assess neocollagenesis.
Results: Both evaluators reported statistically significant improvements compared with baseline for each item on the cellulite severity scale (P < 0.001) with a 4.5-point improvement in mean overall score (P < 0.001) after a single MFU-V/CaHA treatment. At 90 days, histologic analysis showed peak neocollagenesis in samples treated with the 1:1 dilution, whether with CaHA alone or in combination with MFU-V. The highest conversion of collagen type III into collagen type I at month 3 occurred in samples injected with 1:1 and 1:0.6 CaHA dilutions without subsequent MFU-V treatment. Both procedures were well tolerated, and subject satisfaction was high.
Conclusions: Combination treatment with MFU-V and diluted CaHA is effective for improving skin laxity and the appearance of cellulite on the buttocks and upper thighs.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by Merz Pharmaceuticals GmbH.
Figures
References
-
- Luebberding S, Krueger N, Sadick NS. Cellulite: an evidence-based review. Am J Clin Dermatol. 2015;16:243–256.. - PubMed
-
- Lorencini M, Camozzato F, Hexsel D. Farage MA, Miller KW, Maibach HI. Skin aging and cellulite in women. In: Textbook of Aging Skin. 2016:Berlin, Germany: Springer; 1–9..
-
- Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4:221–229.. - PubMed
-
- Mirrashed F, Sharp JC, Krause V, et al. Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite grading. Skin Res Technol. 2004;10:161–168.. - PubMed
-
- Hexsel D, de Oliveira Dal’Forno T, Cignachi S. Goldman MP, Bacci PA, Leibaschoff G, Hexsel D, Angelini F. Definition, clinical aspects, associated conditions, and differential diagnosis. In: Cellulite Pathophysiology and Treatment. 2006:New York, N.Y.: Taylor and Francis Group; 7–27..
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical