

Screening for type 2 diabetes: do screen-detected cases fare better?
- PMID: 28831538
- PMCID: PMC6086324
- DOI: 10.1007/s00125-017-4402-4
Screening for type 2 diabetes: do screen-detected cases fare better?
Abstract
Aims/hypothesis: We aimed to investigate whether diabetes cases detected through screening have better health outcomes than clinically detected cases in a population-based cohort of adults who were eligible to be screened for diabetes at 10 year intervals.
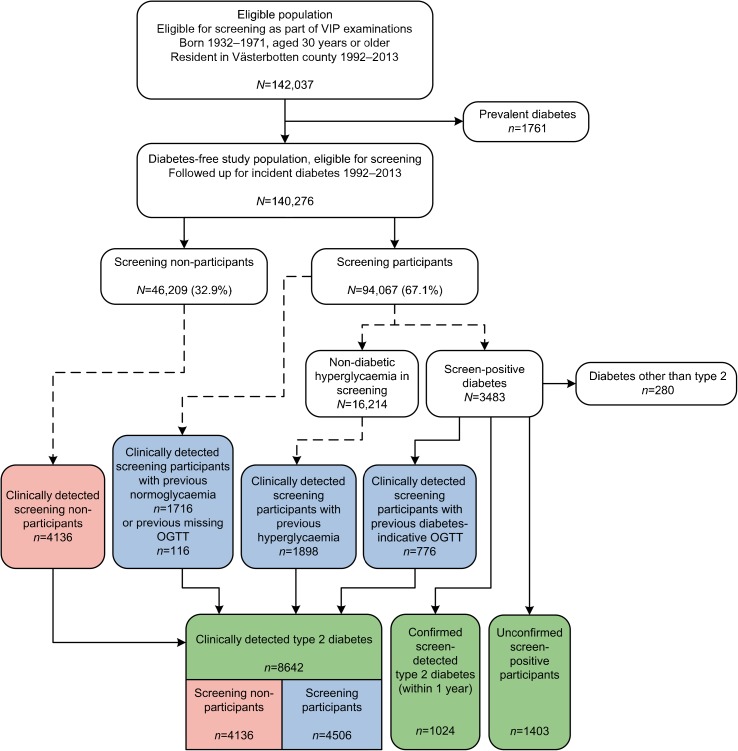
Methods: The Västerbotten Intervention Programme is a community- and individual-based public health programme in Västerbotten County, Sweden. Residents are invited to clinical examinations that include screening for diabetes by OGTTs at age 30, 40, 50 and 60 years (individuals eligible for screening, n = 142,037). Between 1992 and 2013, we identified 1024 screen-detected cases and 8642 clinically detected cases of diabetes using registry data. Clinically detected individuals were either prior screening participants (n = 4506) or people who did not participate in screening (non-participants, n = 4136). Study individuals with diabetes were followed from date of detection until end of follow-up, emigration, death or incident cardiovascular disease (CVD), renal disease or retinopathy event, and compared using Cox proportional hazard regression adjusted for calendar time, age at detection, year of detection, sex and socioeconomic status.
Results: The average age at diabetes diagnosis was 4.6 years lower for screen-detected individuals compared with clinically detected individuals. Overall, those who were clinically detected had worse health outcomes than those who were screen-detected (HR for all-cause mortality 2.07 [95% CI 1.63, 2.62]). Compared with screen-detected study individuals, all-cause mortality was higher for clinically detected individuals who were screening non-participants (HR 2.31 [95% CI 1.82, 2.94]) than for those clinically detected who were prior screening participants (HR 1.70 [95% CI 1.32, 2.18]). Estimates followed a similar pattern for CVD, renal disease and retinopathy.
Conclusions/interpretation: Individuals with screen-detected diabetes were diagnosed earlier and appeared to fare better than those who were clinically detected with regard to all-cause mortality, CVD, renal disease and retinopathy. How much of these associations can be explained by earlier treatment because of screening rather than healthy user bias, lead time bias and length time bias warrants further investigation.
Keywords: Diabetes mellitus; Early diagnosis; Epidemiology; Mass screening; Public health.
Conflict of interest statement
Data availability
Data from the Västerbotten Intervention Study may be obtained from the corresponding author on reasonable request; all linked datasets may be obtained separately from the various register holders, as listed in the Methods section.
Duality of interest
SJG declares receipt of an honorarium and reimbursement of travel expenses from Eli Lilly associated with membership of an independent data-monitoring committee for a randomised trial of a medication to lower glucose, and receipt of honoraria for speaking at postgraduate educational meetings from Janssen and Astra Zeneca. All other authors declare no duality of interest associated with this manuscript.
Contribution statement
ALF designed the analysis plan, performed the data analyses, interpreted the results and drafted and critically revised the manuscript. OR conceived the study question, obtained the data, contributed to the analysis plan, interpreted the results and critically revised the manuscript. SJG contributed to the analysis plan, interpreted the results and critically revised the manuscript. LW and MN coordinated the data collection in the Västerbotten Intervention Study, contributed to the analysis plan and critically revised the manuscript. EF and PW contributed to the analysis plan and critically revised the manuscript. All authors have approved the final version of the manuscript. OR is the guarantor of this work.
Figures
References
-
- International Diabetes Federation (2015) IDF diabetes atlas, 7th edn. Available from www.diabetesatlas.org/. Accessed 31 July 2017
-
- Simmons RK, Griffin SJ, Witte DR, Borch-Johnsen K, Lauritzen T, Sandbæk A (2017) Effect of population screening for type 2 diabetes and cardiovascular risk factors on mortality rate and cardiovascular events: a controlled trial among 1,912,392 Danish adults. Diabetologia DOI 10.1007/s00125-017-4323-2 - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
