

The impact of patient-specific instrumentation on unicompartmental knee arthroplasty: a prospective randomised controlled study
- PMID: 28831554
- PMCID: PMC5966491
- DOI: 10.1007/s00167-017-4677-5
The impact of patient-specific instrumentation on unicompartmental knee arthroplasty: a prospective randomised controlled study
Abstract
Purpose: Patient-specific instrumentation (PSI) has been proposed as a means of improving surgical accuracy and ease of implantation during technically challenging procedures such as unicompartmental knee arthroplasty (UKA). The purpose of this prospective randomised controlled trial was to compare the accuracy of implantation and functional outcome of mobile-bearing medial UKAs implanted with and without PSI by experienced UKA surgeons.
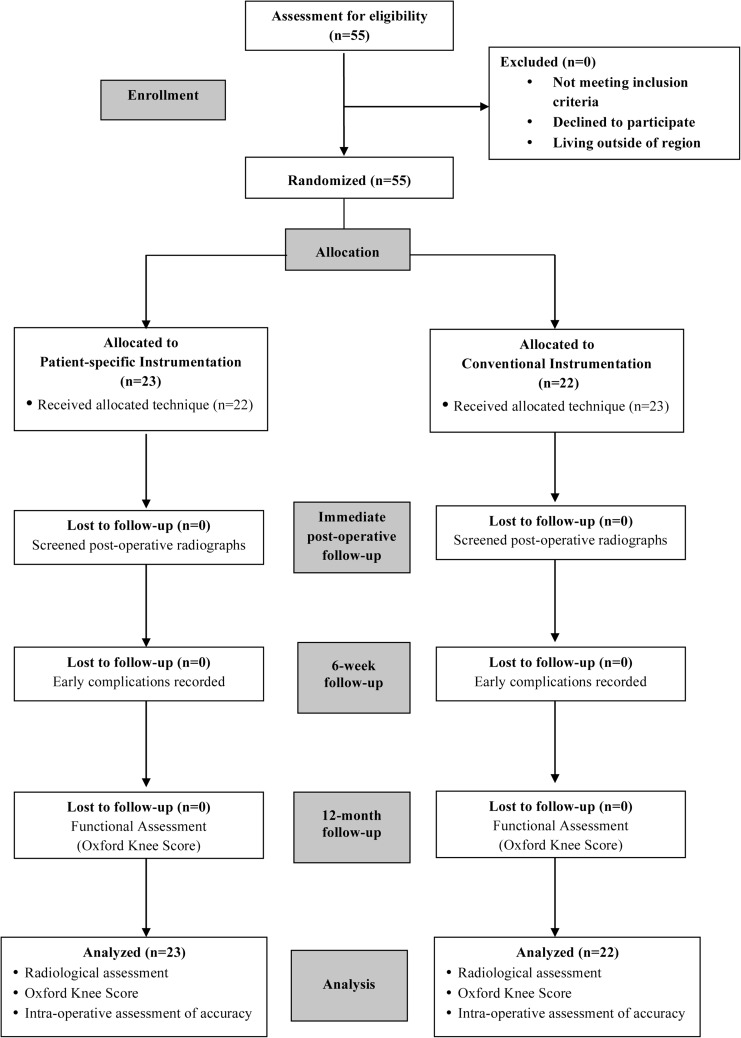
Methods: Mobile-bearing medial UKAs were implanted in 43 patients using either PSI guides or conventional instrumentation. Intra-operative measurements, meniscal bearing size implanted, and post-operative radiographic analyses were performed to assess component positioning. Functional outcome was determined using the Oxford Knee Score (OKS).
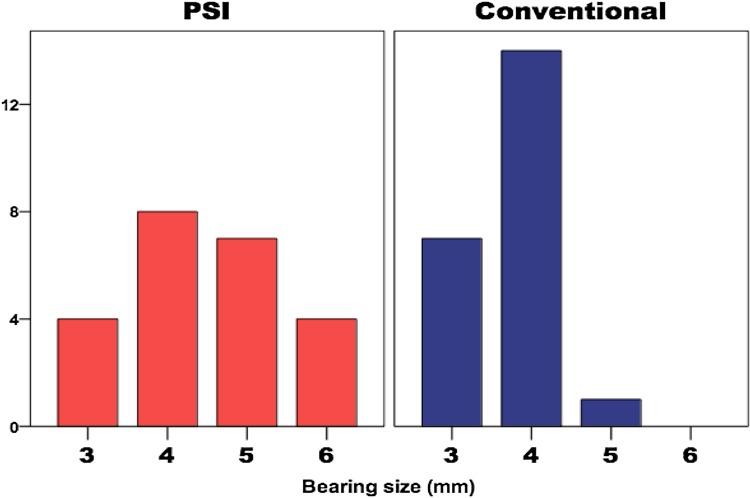
Results: PSI guides could not be used in three cases due to concerns regarding accuracy and registration onto native anatomy, particularly on the tibial side. In general, similar component alignment and positioning was achieved using the two systems (n.s. for coronal/sagittal alignment and tibial coverage). The PSI group had greater tibial slope (p = 0.029). The control group had a higher number of optimum size meniscal bearing inserted (95 vs 52%; p = 0.001). There were no differences in OKS improvements (n.s).
Conclusion: Component positioning for the two groups was similar for the femur but less accurate on the tibial side using PSI, often with some unnecessarily deep resections of the tibial plateau. Although PSI was comparable to conventional instrumentation based on OKS improvements at 12 months, we continue to use conventional instrumentation for UKA at our institution until further improvements to the PSI guides can be demonstrated.
Level of evidence: Therapeutic, Level I.
Keywords: Arthroplasty; Knee; Patient-specific instrumentation; Unicompartmental knee arthroplasty.
Conflict of interest statement
Conflict of interest
The author or one or more of the authors have received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article. In addition, benefits have been or will be directed to a research fund, foundation, educational institution, or other non-profit organisation with which one or more of the authors are associated.
Funding
This study has been supported by the National Institute of Health Research Oxford Biomedical Research Unit.
Ethical approval
For this study ethical approval was obtained, and the trial was registered with the United Kingdom National Research Ethics Service committee (REC reference: 11/H0605/1).
Figures
Similar articles
-
Superior femoral component alignment can be achieved with Oxford microplasty instrumentation after minimally invasive unicompartmental knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2017 Mar;25(3):729-735. doi: 10.1007/s00167-016-4173-3. Epub 2016 May 25. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27225890 Clinical Trial.
-
The John Insall Award: No Functional Benefit After Unicompartmental Knee Arthroplasty Performed With Patient-specific Instrumentation: A Randomized Trial.Clin Orthop Relat Res. 2016 Jan;474(1):60-8. doi: 10.1007/s11999-015-4259-0. Clin Orthop Relat Res. 2016. PMID: 25791446 Free PMC article. Clinical Trial.
-
Patient-specific instrumentation in Oxford unicompartmental knee arthroplasty is reliable and accurate except for the tibial rotation.Knee Surg Sports Traumatol Arthrosc. 2018 Jun;26(6):1823-1830. doi: 10.1007/s00167-017-4826-x. Epub 2017 Dec 27. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 29282486
-
Accuracy and early outcomes in medial unicompartmental knee arthroplasty performed using patient specific instrumentation.Knee. 2014;21 Suppl 1:S33-6. doi: 10.1016/S0968-0160(14)50007-5. Knee. 2014. PMID: 25382366 Review.
-
Patient-specific instrumentation does not improve radiographic alignment or clinical outcomes after total knee arthroplasty.Acta Orthop. 2016 Aug;87(4):386-94. doi: 10.1080/17453674.2016.1193799. Epub 2016 Jun 1. Acta Orthop. 2016. PMID: 27249110 Free PMC article. Review.
Cited by
-
Radiological outcomes following manual and robotic-assisted unicompartmental knee arthroplasty.Bone Jt Open. 2021 Mar;2(3):191-197. doi: 10.1302/2633-1462.23.BJO-2020-0205.R1. Bone Jt Open. 2021. PMID: 33739128 Free PMC article.
-
Patient-specific instrumentation does not improve tibial component coronal alignment for medial UKA compared to conventional instrumentation.J Exp Orthop. 2020 Jun 8;7(1):42. doi: 10.1186/s40634-020-00257-3. J Exp Orthop. 2020. PMID: 32514889 Free PMC article.
-
Do patient-specific instruments (PSI) for UKA allow non-expert surgeons to achieve the same saw cut accuracy as expert surgeons?Arch Orthop Trauma Surg. 2018 Nov;138(11):1601-1608. doi: 10.1007/s00402-018-3031-9. Epub 2018 Sep 3. Arch Orthop Trauma Surg. 2018. PMID: 30178169 Free PMC article.
-
No advantage for patient-specific UKA in comparison with standard UKA regarding clinical and functional results at short-term follow-up.Eur J Orthop Surg Traumatol. 2025 Aug 27;35(1):362. doi: 10.1007/s00590-025-04467-2. Eur J Orthop Surg Traumatol. 2025. PMID: 40866508 Free PMC article.
-
Comparing clinical and radiographic outcomes of robotic-assisted, computer-navigated and conventional unicompartmental knee arthroplasty: A network meta-analysis of randomized controlled trials.J Orthop. 2021 May 13;25:212-219. doi: 10.1016/j.jor.2021.05.012. eCollection 2021 May-Jun. J Orthop. 2021. PMID: 34045825 Free PMC article. Review.
References
-
- Baker P, Jameson S, Critchley R, Reed M, Gregg P, Deehan D. Center and surgeon volume influence the revision rate following unicondylar knee replacement: an analysis of 23,400 medial cemented unicondylar knee replacements. J Bone Joint Surg Am. 2013;95:702–709. doi: 10.2106/JBJS.L.00520. - DOI - PubMed
-
- Bruni D, Iacono F, Russo A, Zaffagnini S, Marcheggiani Muccioli GM, Bignozzi S, et al. Minimally invasive unicompartmental knee replacement: retrospective clinical and radiographic evaluation of 83 patients. Knee Surg Sports Traumatol Arthrosc. 2010;18:710–717. doi: 10.1007/s00167-009-0895-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
