

A Pilot Randomized Controlled Trial of an Integrated In-person and Mobile Phone Delivered Counseling and Text Messaging Intervention to Reduce HIV Transmission Risk among Male Sex Workers in Chennai, India
- PMID: 28831618
- PMCID: PMC5784829
- DOI: 10.1007/s10461-017-1884-5
A Pilot Randomized Controlled Trial of an Integrated In-person and Mobile Phone Delivered Counseling and Text Messaging Intervention to Reduce HIV Transmission Risk among Male Sex Workers in Chennai, India
Abstract
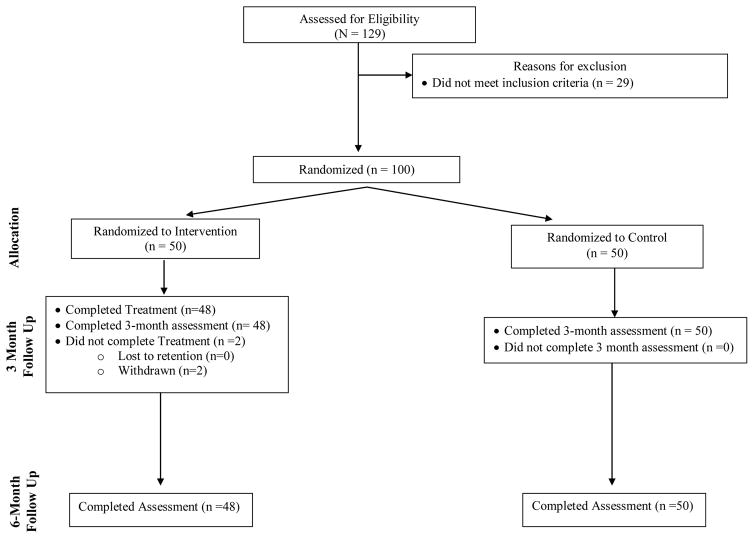
Men who have sex with men (MSM) are at increased risk for HIV infection in India, particularly those who engage in transactional sex with other men (i.e., male sex workers; MSW). Despite the need, HIV prevention efforts for Indian MSW are lacking. As in other settings, MSW in India increasingly rely on the use of mobile phones for sex work solicitation. Integrating mobile phone technology into an HIV prevention intervention for Indian MSW may mitigate some of the challenges associated with face-to face approaches, such as implementation, lack of anonymity, and time consumption, while at the same time proving to be both feasible and useful. This is a pilot randomized controlled trial to examine participant acceptability, feasibility of study procedures, and preliminary efficacy for reducing sexual risk for HIV. MSW (N = 100) were equally randomized to: (1) a behavioral HIV prevention intervention integrating in-person and mobile phone delivered HIV risk reduction counseling, and daily, personalized text or voice messages as motivating "cognitive restructuring" cues for reducing condomless anal sex (CAS); or (2) a standard of care (SOC) comparison condition. Both groups received HIV counseling and testing at baseline and 6-months, and completed ACASI-based, behavioral and psychosocial assessments at baseline, 3, and 6 months. Mixed-effects regression procedures specifying a Poisson distribution and log link with a random intercept and slope for month of follow-up was estimated to assess the intervention effect on the primary outcomes: (1) CAS acts with male clients who paid them for sex, and (2) CAS acts with male non-paying sexual partners-both outcomes assessed over the past month. The intervention was both feasible (98% retention at 6-months) and acceptable (>96% of all intervention sessions attended); all intervention participants rated the intervention as "acceptable" or "very acceptable." A reduction in the reported number of CAS acts with male clients who paid them for sex in the past month was seen in both study conditions. MSW in the intervention condition reported a faster rate of decline in the number of CAS acts with male clients in the past month from the baseline to both the 3-month (B = -1.20; 95% CI -1.68, -0.73; p < 0.0001) and 6-month (B = -2.44; 95% CI -3.35, -1.53; p < 0.00001) assessment visits compared to the SOC condition. Post-hoc contrasts indicated that, at 3 months, participants in the intervention condition reported 1.43 (SD = 0.29) CAS acts with male clients in the past month compared to 4.85 (SD = 0.87) in the control condition (p = 0.0003). Furthermore, at 6 months, the intervention condition participants reported 0.24 (SD = 0.09) CAS acts with male clients in the past month compared to 2.79 (SD = 0.79) in the control condition (p < 0.0001). Findings are encouraging and provide evidence of feasibility and acceptability, and demonstrate initial efficacy (for reducing sexual risk for HIV) of a behavioral HIV prevention intervention for Indian MSW that combines daily, personalized text or voice messages with mobile phone-delivered sexual risk reduction counseling and skills building. Future testing of the intervention in a fully powered randomized controlled efficacy trial is warranted.
Keywords: Behavioral intervention; HIV; HIV prevention; India; Male sex workers (MSW); Men who have sex with men (MSM).
Similar articles
-
Development and Open Pilot Trial of an HIV-Prevention Intervention Integrating Mobile-Phone Technology for Male Sex Workers in Chennai, India.Arch Sex Behav. 2017 May;46(4):1035-1046. doi: 10.1007/s10508-015-0665-3. Epub 2015 Dec 29. Arch Sex Behav. 2017. PMID: 26714684 Free PMC article.
-
A Randomized Pilot Study of a Group-Delivered HIV Risk Reduction Intervention for At-Risk Urban Men Who Have Sex with Men Who Regularly Attend Private Sex Events.Arch Sex Behav. 2019 May;48(4):1059-1071. doi: 10.1007/s10508-018-1326-0. Epub 2019 Feb 25. Arch Sex Behav. 2019. PMID: 30805830 Clinical Trial.
-
Strengthening resilience to reduce HIV risk in Indian MSM: a multicity, randomised, clinical efficacy trial.Lancet Glob Health. 2021 Apr;9(4):e446-e455. doi: 10.1016/S2214-109X(20)30547-7. Lancet Glob Health. 2021. PMID: 33740407 Free PMC article. Clinical Trial.
-
A systematic review and meta-analysis in the effectiveness of mobile phone interventions used to improve adherence to antiretroviral therapy in HIV infection.BMC Public Health. 2019 Jul 9;19(1):915. doi: 10.1186/s12889-019-6899-6. BMC Public Health. 2019. PMID: 31288772 Free PMC article.
-
A systematic review of mHealth interventions for HIV prevention and treatment among gay, bisexual, and other men who have sex with men.Transl Behav Med. 2020 Oct 12;10(5):1211-1220. doi: 10.1093/tbm/ibaa007. Transl Behav Med. 2020. PMID: 33044531 Free PMC article.
Cited by
-
An Internet-Based Self-Testing Model (Easy Test): Cross-Sectional Survey Targeting Men Who Have Sex With Men Who Never Tested for HIV in 14 Provinces of China.J Med Internet Res. 2019 May 15;21(5):e11854. doi: 10.2196/11854. J Med Internet Res. 2019. PMID: 31094339 Free PMC article.
-
Unintended Consequences of mHealth Interactive Voice Messages Promoting Contraceptive Use After Menstrual Regulation in Bangladesh: Intimate Partner Violence Results From a Randomized Controlled Trial.Glob Health Sci Pract. 2019 Sep 26;7(3):386-403. doi: 10.9745/GHSP-D-19-00015. Print 2019 Sep. Glob Health Sci Pract. 2019. PMID: 31558596 Free PMC article. Clinical Trial.
-
The Effectiveness of Electronic Health Interventions for Promoting HIV-Preventive Behaviors Among Men Who Have Sex With Men: Meta-Analysis Based on an Integrative Framework of Design and Implementation Features.J Med Internet Res. 2020 May 25;22(5):e15977. doi: 10.2196/15977. J Med Internet Res. 2020. PMID: 32449685 Free PMC article. Review.
-
Economic evaluation of short message service intervention for HIV prevention among men who have sex with men in China: a modelling study.BMC Public Health. 2024 Dec 20;24(1):3553. doi: 10.1186/s12889-024-20857-3. BMC Public Health. 2024. PMID: 39707268 Free PMC article.
-
Sexual behaviour change following HIV testing services: a systematic review and meta-analysis.J Int AIDS Soc. 2020 Nov;23(11):e25635. doi: 10.1002/jia2.25635. J Int AIDS Soc. 2020. PMID: 33161636 Free PMC article.
References
-
- Department of AIDS Control - Ministry of Health & Family Welfare. Annual Report 2012–2013. India: Department of AIDS Control - National AIDS Control Organization; 2012.
-
- Mimiaga MJ. Differential HIV transmission risk behaviors among MSM subgroups engaging in transactional sex in Chennai, India. Presentation presented at; 2010; International AIDS Society Meeting; Vienna, Austria.
-
- Shinde S, Setia MS, Row-Kavi A, Anand V, Jerajani H. Male sex workers: Are we ignoring a risk group in Mumbai, India? Indian Journal of Dermatology, Venereology, and Leprology. 2009;75(1):41–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
