

Patterns of uptake of prostate-specific membrane antigen (PSMA)-targeted 18F-DCFPyL in peripheral ganglia
- PMID: 28831739
- PMCID: PMC5651702
- DOI: 10.1007/s12149-017-1201-4
Patterns of uptake of prostate-specific membrane antigen (PSMA)-targeted 18F-DCFPyL in peripheral ganglia
Abstract
Objective: Radiotracers targeting prostate-specific membrane antigen (PSMA) have increasingly been recognized as showing uptake in a number of normal structures, anatomic variants, and non-prostate-cancer pathologies. We aimed to explore the frequency and degree of uptake in peripheral ganglia in patients undergoing PET with the PSMA-targeted agent 18F-DCFPyL.
Methods: A total of 98 patients who underwent 18F-DCFPyL PET/CT imaging were retrospectively analyzed. This included 76 men with prostate cancer (PCa) and 22 patients with renal cell carcinoma (RCC; 13 men, 9 women). Scans were evaluated for uptake in the cervical, stellate, celiac, lumbar and sacral ganglia. Maximum standardized uptake value corrected to body weight (SUVmax), and maximum standardized uptake value corrected to lean body mass (SULmax) were recorded for all ganglia with visible uptake above background. Ganglia-to-background ratios were calculated by dividing the SUVmax and SULmax values by the mean uptake in the ascending aorta (Aortamean) and the right gluteus muscle (Gluteusmean).
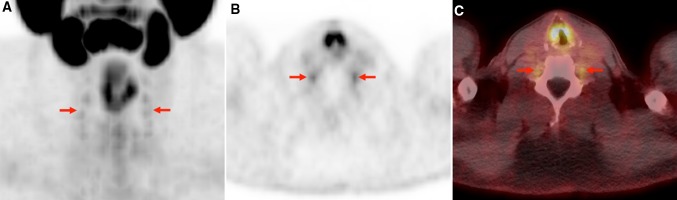
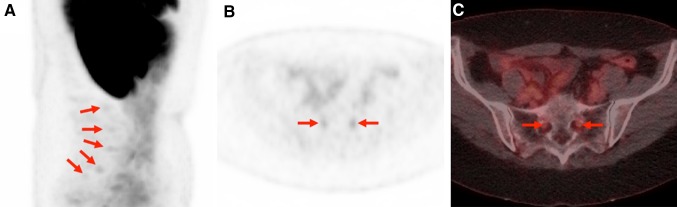
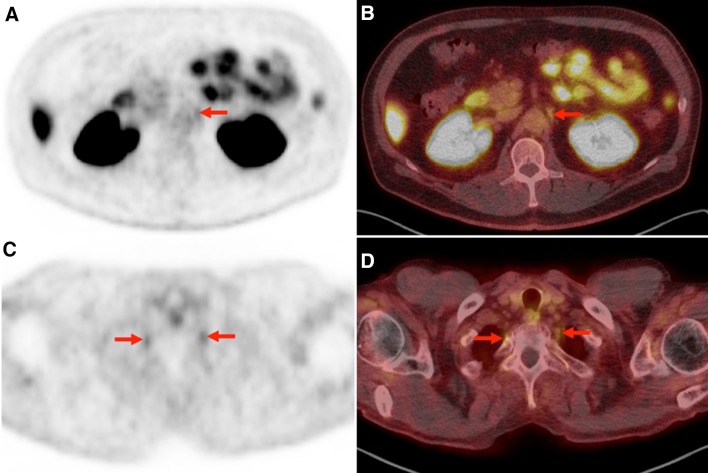
Results: Overall, 95 of 98 (96.9%) patients demonstrated uptake in at least one of the evaluated peripheral ganglia. With regard to the PCa cohort, the most frequent sites of radiotracer accumulation were lumbar ganglia (55/76, 72.4%), followed by the cervical ganglia (51/76, 67.1%). Bilateral uptake was found in the majority of cases [lumbar 44/55 (80%) and cervical 30/51 (58.8%)]. Additionally, discernible radiotracer uptake was recorded in 50/76 (65.8%) of the analyzed stellate ganglia and in 45/76 (59.2%) of the celiac ganglia, whereas only 5/76 (6.6%) of the sacral ganglia demonstrated 18F-DCFPyL accumulation. Similar findings were observed for patients with RCC, with the most frequent locations of radiotracer uptake in both the lumbar (20/22, 90.9%) and cervical ganglia (19/22, 86.4%). No laterality preference was found in mean PSMA-ligand uptake for either the PCa or RCC cohorts.
Conclusion: As PSMA-targeted agents become more widely disseminated, the patterns of uptake in structures that are not directly relevant to patients' cancers must be understood. This is the first systematic evaluation of the uptake of 18F-DCFPyL in ganglia demonstrating a general trend with a descending frequency of radiotracer accumulation in lumbar, cervical, stellate, celiac, and sacral ganglia. The underlying biology that leads to variability of PSMA-targeted radiotracers in peripheral ganglia is not currently understood, but may provide opportunities for future research.
Keywords: 18F-DCFPyL; Ganglia; Imaging pitfalls; PSMA; Prostate cancer.
Conflict of interest statement
Conflict of interest
MGP is a coinventor on a US Patent covering 18F-DCFPyL, and as such is entitled to a portion of any licensing fees and royalties generated by this technology. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict-of-interest policies. MAG has served as a consultant to Progenics Pharmaceuticals, the licensee of 18F-DCFPyL. MAG, KJP, MGP, and SPR have received research support from Progenics Pharmaceuticals.
Sources of funding
The Prostate Cancer Foundation Young Investigator Award, philanthropy raised by the James Buchanan Brady Urological Institute, and National Institutes of Health Grants CA134675 and CA183031. This project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie Grant agreement.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
