

A randomized, placebo-controlled trial of cenicriviroc for treatment of nonalcoholic steatohepatitis with fibrosis
- PMID: 28833331
- PMCID: PMC5947654
- DOI: 10.1002/hep.29477
A randomized, placebo-controlled trial of cenicriviroc for treatment of nonalcoholic steatohepatitis with fibrosis
Abstract
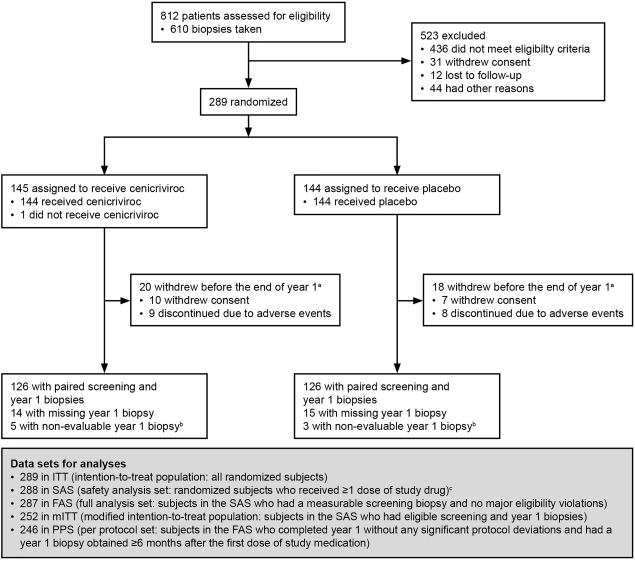
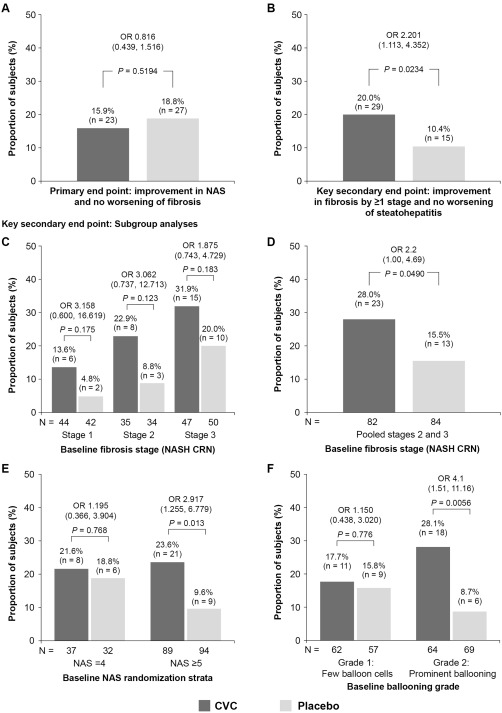
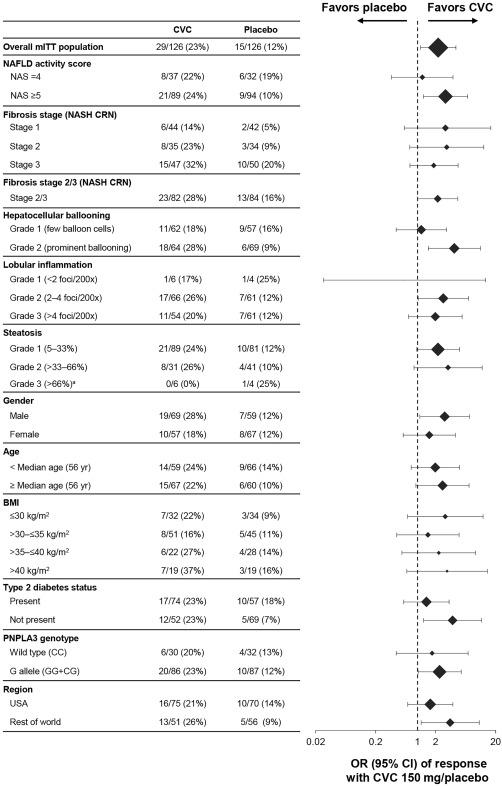
The aim of this study was to evaluate cenicriviroc (CVC), a dual antagonist of CC chemokine receptor types 2 and 5, for treatment of nonalcoholic steatohepatitis (NASH) with liver fibrosis (LF). A randomized, double-blind, multinational phase 2b study enrolled subjects with NASH, a nonalcoholic fatty liver disease activity score (NAS) ≥4, and LF (stages 1-3, NASH Clinical Research Network) at 81 clinical sites. Subjects (N = 289) were randomly assigned CVC 150 mg or placebo. Primary outcome was ≥2-point improvement in NAS and no worsening of fibrosis at year 1. Key secondary outcomes were: resolution of steatohepatitis (SH) and no worsening of fibrosis; improvement in fibrosis by ≥1 stage and no worsening of SH. Biomarkers of inflammation and adverse events were assessed. Full study recruitment was achieved. The primary endpoint of NAS improvement in the intent-to-treat population and resolution of SH was achieved in a similar proportion of subjects on CVC (N = 145) and placebo (N = 144; 16% vs. 19%, P = 0.52 and 8% vs. 6%, P = 0.49, respectively). However, the fibrosis endpoint was met in significantly more subjects on CVC than placebo (20% vs. 10%; P = 0.02). Treatment benefits were greater in those with higher disease activity and fibrosis stage at baseline. Biomarkers of systemic inflammation were reduced with CVC. Safety and tolerability of CVC were comparable to placebo.
Conclusion: After 1 year of CVC treatment, twice as many subjects achieved improvement in fibrosis and no worsening of SH compared with placebo. Given the urgent need to develop antifibrotic therapies in NASH, these findings warrant phase 3 evaluation. (Hepatology 2018;67:1754-1767).
© 2017 The Authors. Hepatology published by Wiley Periodicals, Inc., on behalf of the American Association for the Study of Liver Diseases.
Figures
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease–meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73‐84. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non‐alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am J Gastroenterol 2012;107:811‐826. - PubMed
-
- Ekstedt M, Hagström H, Nasr P, Fredrikson M, Stål P, Kechagias S, et al. Fibrosis stage is the strongest predictor for disease‐specific mortality in NAFLD after up to 33 years of follow‐up. Hepatology 2015;61:1547‐1554. - PubMed
-
- Younossi ZM, Stepanova M, Rafiq N, Makhlouf H, Younoszai Z, Agrawal R, et al. Pathologic criteria for nonalcoholic steatohepatitis: interprotocol agreement and ability to predict liver‐related mortality. Hepatology 2011;53:1874‐1882. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
